Comparison of COVID-19 Prevention Knowledgein Bangladeshi Americans vs. Bangladeshis
Suhaila Khan, Yusuf Mamoon, Syed Moosa
1Research Ambitions-BMANA
2SHK Global Health
3Queens Hospital Center
4SUNY Downstate Medical Center
This survey illustrated some similarities, differences, and gaps in COVID-19 prevention knowledge of people living in a developed (US) and a developing (Bangladesh) country. Population-based data were collected with bilingual (English, Bangla) online surveys during February-March 2020 from Bangladeshi Americans living in the US and Bangladeshis living in Bangladesh. There were 1,604 study respondents (US=850, BD=754).
Knowledge about preventive measures were significantly higher in the US compared to Bangladesh, e.g., handwash (US 98%,BD 92%), cover cough (US 93%, BD 83%), stay home if sick (US 89%, BD 71%). Majority (US 52%, BD73%)of the respondents said that it was difficult to find reliable information.
In the US, the main sources of information were CDC 38%, social media 35%, and TV 14%. In Bangladesh, the main sources of information were social media 53%, WHO-NHS 21%, and IEDCR 10%. Only 3% respondents received information from physicians and <1% from faith-based organizations, in US and Bangladesh. More respondents in the US compared to Bangladesh said that home and all types of institutions (health facility, K12 school) were responsible for taking preventive action.
Physicians and faith-based organizations were not sources of information in US or Bangladesh; they need to be. The US needs to improve access to culturally and linguistically appropriate information from the CDC. Bangladesh needs to urgently improve IEDCR’s communications efforts as most respondents replied relying on social media and non-Bangladeshi institutions for information. Bangladesh also needs to utilize academic institutions (K-12 to university) as sources of information.
Keyword: COVID-19 prevention knowledge Bangladeshi American
Comparison of COVID-19 Prevention Knowledgein Bangladeshi Americans vs. Bangladeshis
Suhaila Khan, Yusuf Mamoon, Syed Moosa
1Research Ambitions-BMANA
2SHK Global Health
3Queens Hospital Center
4SUNY Downstate Medical Center
INTRODUCTION
Background
Coronavirus Disease 2019 (COVID-19) is a respiratory disease in humans caused by a virus named Severe Acute Respiratory Syndrome Coronavirus 2 (SARS- CoV-2).1-2 It was very contagious and spread quickly around the world, and caused a global pandemic in 2020 with very high morbidity and mortality everywhere in the world, developed and developing. The World Health Organization (WHO) declared it a pandemic in March 2020.3
Physicians of the Bangladesh Medical Association of North America (BMANA) were receiving many questions about COVID-19 from both Bangladeshi Americans in the United States (US) and Bangladeshis in Bangladesh (BD) from very early in 2020. To address the community’s questions, a survey in these two population groups was deemed urgent.
Bangladeshis are people who live and work in Bangladesh. Bangladeshi Americans are people of Bangladeshi descent who live and work in the United States (US). These two population groups are culturally and linguistically similar,and were affected by COVID-19 at the same time. But one group lives in a developed country and the other group lives in a developing country with significant differences in terms of choices and opportunities in access to healthcare, economic opportunities, food, housing, transportation, etc. For example, Bangladeshi Americans need health insurance to access healthcare in the US, whereas in Bangladesh it is usually out-of-pocket with limited public services. There are 208,000 Bangladeshi Americans (US total population 332 million), and 169 million people in Bangladesh. Per capita income in US is $37,638 and in Bangladesh $2,457.4-10
Compared to other immigrant communities in the US, Bangladeshi Americans had the top ten uninsured population (3rd highest at 12.9%), limited English proficiency (4th highest at 43.2%), low high school education (9th highest at 15.9%), and foreign-born population (3rd highest at 74.3%). All these rates were worse at state and city levels compared to the national level.8 Bangladeshi Americans live in all 50 States in the US. The 5 top metropolitan areas for Bangladeshi Americans are: NY, Detroit, Washington, Los Angeles, Philadelphia.6,7
Data are essential for understanding and addressing the gaps and unmet needs in any community – whether in developed or developing country. Data informs prioritizing risks and resources, funding (federal, state, local, international), policy development, program development, and prepare for future pandemics.
Study Objectives
The study objectives were: 1) To assess the knowledge and awareness about the prevention of COVID-19 in Bangladeshi Americans and Bangladeshis. 2) To assess if there are similarities and differences in the two population groups regarding their knowledge and awareness about the prevention of COVID-19.
METHODOLOGY
Study Design, Study Period, Study Location, and Study Participants:
This was a population-based cross-sectional study. Data were collected with a self-administered online survey during February and March 2020. It took 5 minutes to complete the survey. The study participants were Bangladeshi Americans living in the US and Bangladeshis living in Bangladesh.
Survey Instruments:
Two survey questionnaires were created – one for Bangladeshi Americans and one for Bangladeshis. Both questionnaires were bilingual (English and Bangla) to overcome any language barriers. The questionnaires were disseminated through social media (e.g, Facebook, WhatsApp, Messenger), listservs, email, and word of mouth. The questionnaires were structured, close ended; most questions were bimodal (e.g., yes/no options), and some questions had multiple-choice options. Guidelines for use of facemasks were provided by the CDC on 04/03/2020, after the data collection for this study ended.11
Study Variables, Sampling, Sample Size, andData:
The study variables were related to the following characteristics: socio-demographic (e.g., geographic location, gender, age), COVID-19 (e.g., measures that prevent spread of COVID-19, difficulty finding information, source of information, who is responsible for taking preventive action against COVID-19). Convenience sampling strategy was used as this was the first time data were collected simultaneously when movement was extremely restricted in both countries. Data were cleaned, then coded and analyzed. Excel and Stata were used for descriptive and bivariate analysis (Pearson’s chi-squaretest). Sampling weights were not used as this was not a probabilistic sample.
Confidentiality, Privacy, and Informed Consent:
No personal identifying information was collected from the study participants. Informed consent was taken at the start of the surveys. Participation was voluntary and monetary compensations were not provided. This study was reviewed and approved by the Ethical Committee of BMANA.12
STUDY RESULTS
Demographic Characteristics:
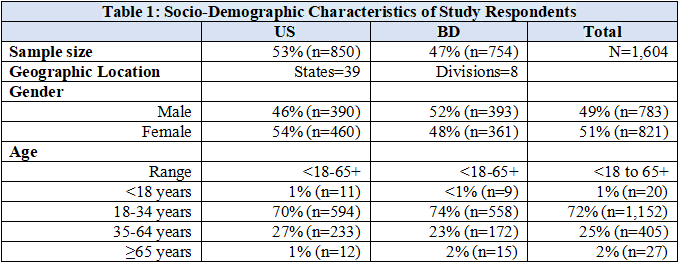
There were N=1,604 survey respondents (Table1). The US sample had more female respondents (M 46%, F54%), and the Bangladesh sample had more male respondents (M 52%, F 48%). The age of the study respondents ranged from <18 years to 65+ years. The majority were ages 18-34 years in both US (70%) and Bangladesh (74%). The age question had 4 options to choose from: below 18 years, 18-34 years, 35-64 years, and 65 years or more.
The study respondents were geographically very diverse from 39 States in the US and 8 Divisions in Bangladesh.The US states with the highest respondents were: NewYork (26%), Florida (13%), California (9%), Michigan/Ohio/Virginia (each 6%), and Texas (4%). The highest Bangladeshi study respondents were from Dhaka (61%), Chittagong (17%), and Sylhet (10%).
Knowledge about Prevention of COVID-19:
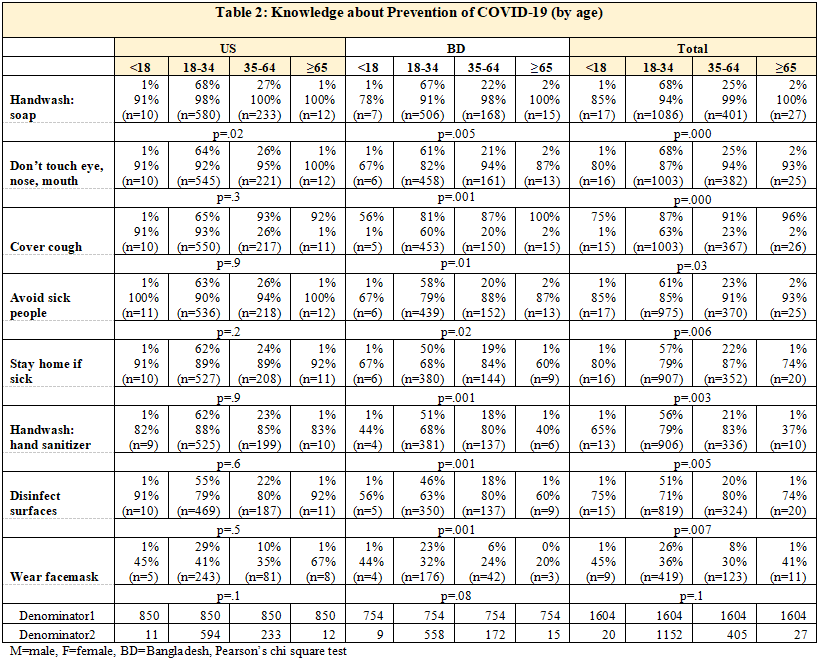
Most study respondents in the US (89%) and Bangladesh (69%) were knowledgeable about 6 or more out of the 8 measures that might prevent the spread of COVID-19 which were: wash hands often with soap; if soap/water not available, use a hand sanitizer; avoid touching eyes, nose, mouth; clean frequently touched surfaces and objects daily; use a face mask when out of home; avoid close contact with people who are sick; stay home when sick; and cover cough or sneeze with a tissue.
Knowledge about all the eight preventive measures were much higher in the US compared to Bangladesh (Figure 1b), e.g., handwash (US 98%, BD 92%), cover cough (US 93%, BD 83%), stay home if sick (US 89%, BD 71%), wear facemask (US 40%, BD 30%). Less than half the study respondents were knowledgeable about ‘wearing a face mask’ both in the US and Bangladesh. The differences were statistically significant for all the knowledge variables (p=.000). A separate question on ‘knowledge of social distancing at 6 feet’ also showed high rates of knowledge (US 94%, Bangladesh 81%); and the differences were statistically significant (p=.000). Data table not shown.
Study participants across all the age groups showed very high levels of knowledge about prevention measures of COVID-19 (Table 2). These differences were statistically significant (p<.05, except for facemask), especially for the Bangladesh respondents. However, for US respondents only handwash with soap was statistically significant for all ages. More women in US and more men in Bangladesh had higher knowledge about the prevention measures of COVID-19. The gender differences were not statistically significant in US or Bangladesh.
.png)
Difficulty Finding Reliable Information:
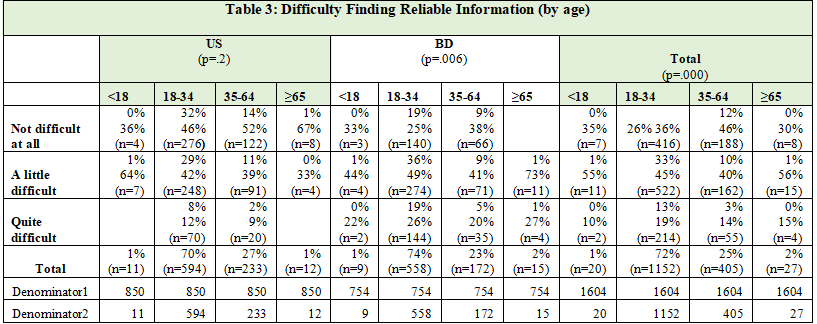
The majority (US 52%, BD 73%) of the respondents said that it was difficult (little and quite) to find reliable information on how to prevent COVID-19 (Figure 2). The Bangladesh respondents had much more difficulty than the US respondents. These differences were statistically significant (p=.000).
.png)
Most study participants across all the age groups said that they had this difficulty (little or quite) finding reliable information (Table 3). In Bangladesh, all the ≥65 years old study respondents reported difficulty (little or quite) finding information; but in the US this age group had only a little difficulty. Age was statistically significant for this outcome for overall sample and in Bangladesh but not in the US. More women reported difficulty in US, and more men in Bangladesh reported difficulty; the differences were not statistically significant.
Main Sources of Information:
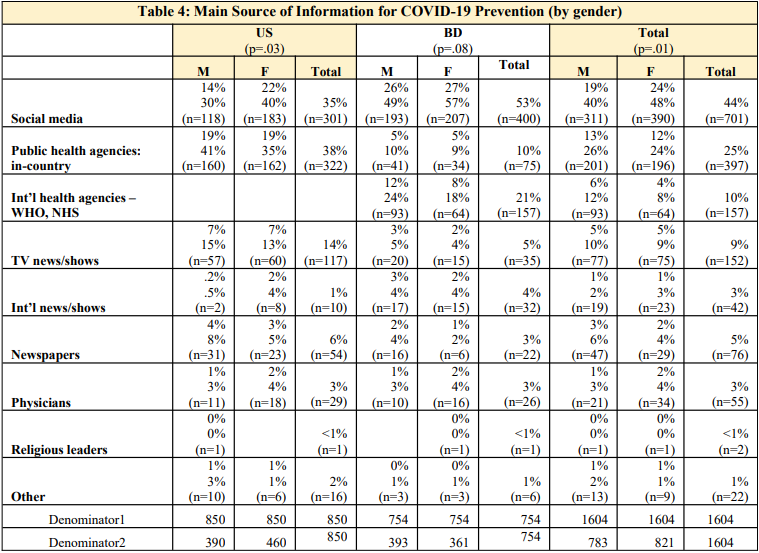
In the US, the main sources of information were public health institution CDC 38%, social media 35%, and TV 14%. In Bangladesh, the main sources of information were social media 53%, international public health institutions WHO and UK’s NHS 21%, and public health institution IEDCR 10%. Reliance on social media was astonishingly high in Bangladesh. These differences were statistically significant (p=.000). In both US and Bangladesh, the study respondents said that they received the least information from physicians (3%) and religious leaders (<1%). Religious leaders are people who are associated with faith-based organizations (e.g.,mosque, temple, church). (Figure 3).
.png)
More women depended on social media for information, both in the US and Bangladesh. More men used public health agency websites to get information, e.g., the CDC in US, and WHO/NHS in Bangladesh (Table4).‘Gender’ was statistically significant with this outcome.
Most study respondents across all the age groups used social media and public health agencies to get their information in the US and in Bangladesh. However, a third of the ≥65 age group also relied on TV news/programs from their respective countries for information. This indicates that even though social media is prominent, traditional sources like TV was still relevant for finding information. The <18 year old group used public health agencies the least, and the ≥65 age group used social media the least. 'Age’ was statistically significant with this outcome. Data table not shown.
Which Entity Should Take Action for Preventing Spread of COVID-19:
More respondents in the US compared to Bangladesh said that home and all types of institutions were responsible for taking action to prevent COVID-19, e.g., home (US 86%, BD 71%), health facility (US 89%, BD 91%), workplace (US 86%, BD 61%), university (US 82%, BD 61%), K-12 schools (US 78%, BD57%), and faith-based organizations (US 70%, BD 49%). These differences were statistically significant for all the outcomes for this question (p=.000, except for health facility which was not significant) (Figure 4).
The 18-64 year old respondents think everyone is responsible for taking preventive action. However, the <18 years and >65 year old respondents do not seem to have much of an opinion about this issue. The differences were statistically significant (p<.05). More women in the US and more men in Bangladesh think that preventive action should be taken by everyone. ‘Gender’ was not statistically significant for this outcome. Data table not shown.
.png)
DISCUSSION
Diverse Geographic Distribution of Study Respondents:
Our study respondents were geographically diverse both in the US (from 37 states) and in Bangladesh (from 8 divisions). The study respondents in the US reflected the geographic distribution in the US as per the top states with the highest Bangladeshi Americans – California, New York, and Texas.8 In the only other survey related to COVID-19-social distancing on Bangladeshi Americans and Bangladeshis, only 20% study respondents were from the US.13
A study on impact of COVID-19 on NY Asian Americans had a sample of 1,353 (only 74 were Bangladeshi Americans).14 That study reported that Bangladeshi and Nepali adults reported having high vaccination acceptance rate, but the lowest vaccination rates compared to other Asian subgroups. Bangladeshi Americans had the second highest rate of language barriers and insufficient access to interpreters and written materials in their preferred language, which poses barriers to accessing health care resources.
A study on South Asian Americans reported that Bangladeshis make up 8% of the NY Asian American population, yet suffered 20% of the deaths related to COVID-19 (secondary data); they also collected primary data from 400 community members but did not provide details about race/ethnicity.15 Bangladeshi Americans in NY also had higher hospitalization rates.16
Gender Balance of Study Respondents:
Compared to the other studies, our study sample had better gender distribution. It was similar to the other study (51%-54%).13 However, studies with other Asian Americans reported much higher female study respondents ranging from 60%-79%.14,17
Study Respondents Mostly Young Adults:
The majority (US 74%, BD 70%, overall 72%) of our study respondents in both countries were ages 18-34 years. This may be because of the online surveys; usually more younger people use the internet and social media. Studies on other Asian Americans either had a high percentage of 18-34 year old respondents in their studies (66%-78%) or did not report the age distribution of their respondents.13-17
Lot of Knowledge about Prevention of COVID-19:
The study respondents in both the US and in Bangladesh were knowledgeable about the specific measures that might prevent the spread of COVID-19 (e.g., washing hands with soap, avoid sick people, stay home if sick, don’t touch nose/mouth). Most respondents mentioned 6 or more answers out of the 8 choices given. Most preventive actions (except face masks) were known to most of the respondents in the US and in Bangladesh – the percentage was much higher in the US respondents.
One study had similar findings in US and UK where people thought COVID-19 could be prevented by washing hands, avoiding sick people, avoiding touching eyes, nose, and mouth with unwashed hands, wearing common surgical mask.18 The study reported a lot of misinformation too: e.g., not eating at Chinese restaurants, using a hand dryer, rinsing nose with saline, taking antibiotics, and gurgling with mouthwash.
Difficulty Finding Reliable Information:
Most respondents in our study said that it was difficult to gather information, by both men and women, and across all the age groups. Other studies also reported that people knew a lot about COVID-19.19,20 However, there was also uncertainty about the reliability of information even though there was high digital literacy.20
Main Sources of Information:
The main “Source of Information” was social media (e.g., YouTube, Facebook, Twitter) in both US and Bangladesh. It was astonishingly high for Bangladesh. The second largest source of information was public health organizations like the CDC (in the US) and WHO (in Bangladesh). Visibility of local public health organization in Bangladesh was very low at the time of this study. The data shows how global the lives of the study respondents have become – US study respondents were tuning into Bangladeshi news, and Bangladesh study respondents were looking for information on CDC, WHO, and NHS websites. Even in the US, social media was used more often than a public health organization like the CDC.
In both countries, the study respondents received the least information from physicians and religious leaders. Other studies also reported lack of messaging from medical community.21,22
More women got their information from social media, both in the US and Bangladesh. More men got their information from public websites like the CDC (in the US), and WHO and NHS (in Bangladesh). In the US, social media and public agencies were used by all age groups. In Bangladesh, most age groups used mostly social media for information. The seniors in both countries are still using traditional media (TV news, newspaper). The <18 year old group used public health agencies the least, and the ≥65 age group used social media the least.
Other studies have also reported social media as a predominant information source for COVID-19, COVID-19 vaccines, etc. – both information and misinformation.21 One qualitative study reported that their respondents found information from TV, family/friends, social media, newspapers, and government websites.14 The study also reported that Asian Americans, including Bangladeshi Americans faced language barriers when accessing information (e.g., long wait time for an interpreter), insufficient written materials in their preferred language, which in turn posed barriers to accessing health care, COVID-19 relief benefits, etc.
Taking Preventive Action is Everybody’s Responsibility--Personal and Institutional:
When asked “who should take action for preventing the spread of COVID-19”, the response was that everyone is responsible – home and institutions (health, educational,work). But the percentages were much higher in the US than in Bangladesh: healthcare facilities, home, K-12schools, universities, workplaces, and faith-based organizations. More women in the US and more men in Bangladesh think that preventive action should be taken by everyone. The 18-64 year olds think everyone is responsible for taking preventive action.
Strengths and Limitations of the Study:
The availability of the internet and social media made data collection relatively easy from both countries during a very difficult time period. The survey was online and social media dependent; and as such may have missed respondents who do not have access to the internet orthose who do not participate in social media. The study did not collect data on some useful indictors, e.g., education,occupation, marital status, and misinformation.
IMPLICATIONS and RECOMMENDATIONS
There are many publications available on the prevention knowledge and impact of COVID-19 on populations in both developed and developing countries.23-27 However, not much data are available on either Bangladeshi Americans living in the US or Bangladeshis living in Bangladesh, let alone a study that compared these two culturally and linguistically similar populations. This study helped bridge some of those gaps.
This study data provide some insight on the COVID-19 prevention knowledge in the early months of the pandemic in 2020 when the disease was still evolving globally. These types of comparison data have implications to better prepare for future global pandemics whether in developed country US or developing country Bangladesh. Such data collection, analysis and reporting are essential to understanding the magnitude of the problem, and identifying resource needs for addressing prevention of spread of communicable infectious diseases.
A) People need information to successfully prevent communicable diseases like COVID-19.
- The US respondents were significantly more knowledgeable about the various measures that prevent COVID-19 compared to respondents in Bangladesh. One reason for this difference may be because the US respondents had better access to information from country-based reliable public health agency. Bangladeshis also had significantly higher difficulty in finding reliable information compared to Bangladeshi Americans.
- It is worrisome that despite living in a developed country like US, half the Bangladeshi American respondents reported difficulty finding reliable information.
B) People need reliable in-country source of information to effectively prevent diseases like COVID-19.
- In the US, the CDC needs to invest more towards the unmet need for access to health related information in people’s preferred language and culture (in this case Bangla). This includes the use of ethnic media (social, digital, print) to communicate with Bangladeshi Americans of all ages.
- In Bangladesh, urgently invest more in its public health agency (IEDCR) and its communications efforts. It is extremely worrisome that most respondents from Bangladesh depended on social media or international organizations like WHO/NHS for life-saving information.
C) Wide availability of the internet andsocial media very prominent source of information in both US and Bangladesh.
- Social media use was astonishingly high in Bangladesh. All institutions (public and private, healthand academic) need to become social media savvy as quickly as possible to address future pandemics, in US and Bangladesh.
- The availability of the internet and social media was equally widespread in the US and in Bangladesh, even though the two countries were economically and geographically very different. This type of study would not have been possible even 5-years ago. Before data collection started, the researchers for our study were unsure of what the response rate would be as this kind of study had not been attempted previously. But to everyone’s surprise the response rates were excellent. This was also probably due to people being housebound during the pandemic.
D) Messaging and messaging outlets need to becountry-specific and age-specific.
- In US and Bangladesh, TV and newspaper are still the main sources of information for seniors.
- In US and Bangladesh, public health agencies need to have more targeted messaging through the various social media outlets.
- In US and Bangladesh, all media (social and traditional) should incorporate information from credible sources (CDC in US, IEDCR in Bangladesh) when developing messages.
E) Absence or lack of involvement of institutions (physicians, faith-based, academic) can affect prevention efforts in a pandemic.
- Physicians and faith-based organizations were the lowest sources of information in both the US and Bangladesh. These two groups are trusted sources and need to be included in messaging efforts from the beginning of any disease outbreaks.
- In Bangladesh, a large student population and their families depend on academic institutions (K-12 to university) for information but did not receiveit. These academic institutions could have been utilized to engage with students with helpful messaging and maintain communications about prevention of COVID-19.
CONCLUSION
This study provided some insights on how to prevent global pandemics from a communicable infectious disease like COVID-19 such as knowledge about preventive measures, access to reliable sources of information, and appropriate preventive messaging. National public health agencies, physicians, faith-based organizations, and academic institutions (K-12 to university) must become more social media savvy with messaging. Physicians and faith-based organizations were not sources of information to people in US or Bangladesh; they need to be. The US needs to improve access to culturally and linguistically appropriate information from the CDC. Bangladesh needs to urgently improve its communications efforts through IEDCR as most respondents there were reliant on social media and non-Bangladeshi international institutions for information. Bangladesh also needs to utilize academic institutions (K-12 to university) as sources of information for youth and their families.
ACKNOWLEDGEMENTS
Many thanks to Dr.s Medha Ghosh, Ashma U. Husna, Sawsan Fathma, Samiya Ali, Hafsa I. Siddiqa, Farjana Nasrin, and Hafiz M. Waliullah for assistance with some preliminary data analysis. Thanks to Fatema Kamal for assistance with the code list. A heartfelt gratitude to the 40+ physicians who disseminated the questionnaires to our communities in the US and Bangladesh.
1. Centers for Disease Control and Prevention. Update and Interim Guidelines on Outbreak of 2019 Novel Coronavirus (2019-nCoV). 2020. Accessed 4/27/20. https://www.cdc.gov/coronavirus/2019ncov/communicati on/guidance-list.html?Sort=Date%3A%3Adesc
2. Centers for Disease Control and Prevention. Basics of COVID-19. 2021. Accessed 6/24/22 https://www.cdc.gov/coronavirus/2019-ncov/your- health/about-covid-19/basics-covid-19.html
3. World Health Organization. Coronavirus Disease (COVID-19) Advice for the Public. Accessed 4/27/20. https://www.who.int/emergencies/diseases/novel- coronavirus-2019/advice-for-public
4. World Bank. Country – Bangladesh. Accessed 3/27/23. https://data.worldbank.org/country/BD
5. AAPI Data. State of Asian Americans, Native Hawaiians, and Pacific Islanders in the United States. 2022.https://aapidata.com/wpcontent/uploads/2022/06/St ate-AANHPIs-National-June2022.pdf
6. Budiman A. Bangladeshis in the US. Factsheet. Pew Research Center. 2021. https://www.pewresearch.org/ social-trends/fact-sheet/asian-americans-bangladeshis-inthe-u-s/
7. Budiman A, Ruiz NG. Key Facts about Asian Americans, A Diverse and Growing Population. PewResearch Center. 2021.https://www.pewresearch.org/facttank/2021/04/29/key-facts-about-asian-americans
8. Khan S. Some Facts about Bangladeshi Americans.National Council of Asian Pacific Islander Physicians.2016. http://ncapip.org/resources/bangladeshi2016report/index.html
9. Migration Policy Institute. The Bangladeshi Diasporainthe United States. RAD Diaspora Profile. 2014.https://www.migrationpolicy.org/sites/default/files/publications/RAD-Bangladesh.pdf
10. South Asian Americans Leading Together (2019).Demographic Snapshot of South Asians in the United States. https://saalt.org/wpcontent/uploads/2019/04/SAALT-Demographic-Snapshot-2019.pdf
11. Centers for Disease Control and Prevention. Use of Cloth Face Coverings to Help Slow the Spreadof COVID-19. 2020. Accessed 4/27/20. https://www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/diy-cloth-face-coverings.html
12. World Medical Association. World Medical Association Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects. JAMA. 2013.310(20):2191–2194. doi:10.1001/jama.2013.281053
13. Sayam S, Dutta P, Sultana N, Agarwala P, etal.Knowledge and Perception of COVID-19 Related Social Distancing Regulations: a Cross-sectional StudyofBangladeshis Living in Bangladesh and the UnitedStates.Global Journal of Infectious Disease. 2022. 2(1). https://www.corpuspublishers.com/assets/articles/gjid-v2-22-1004.pdf
14. NYC COVID-19 CHRNA. NYC COVID-19 Community Resources and Needs Assessment. NYUCenter for the Study of Asian American Health, Coalitionfor Asian American Children and Families, Chinese-AmericanPlanning Council. https://aanhpihealth.org/resource/nyc-covid-19-communityresources-and-needs-assessment-nyc-covid-19-chrna/
15. Hussain M, Qureshi S, Sridaran L, Suryanarayanan S.The Disparate Impact of COVID-19 Across South Asian American Communities. Asian American PolicyReview.2021. 31(2020-21). https://aapr.hkspublications.org/2021/04/16/the-disparateimpact-of-covid-19-across-south-asian-american- communities
16. Marcello RK, Dolle J, Tariq A, Kaur S, etal.Disaggregating Asian Race Reveals COVID-19 Disparitiesamong Asian American Patients at NewYork City'sPublicHospital System. Public Health Rep. 2022;137(2):317-325.doi:10.1177/00333549211061313