Neuro-Endovascular repair of ruptured basilar artery bifurcation aneurysms including those with poor grades: A single center study
Lodi Y ,Babiker A ,Azab M ,Rosenbaum D
BACKGROUND: Endovascular repair of the basilar artery bifurcation ruptured aneurysms (BABRA) is the preferred approach over surgical clipping, as clipping is associated with a higher chance of mortality and morbidity. Additionally, surgical clipping is not offered to those with poor Hunt and Hess grades (H&H). Limited data exists on the outcomes for those with grade IV&V of ruptured BABRA, leading to uncertainty regarding aneurysm repair. The objective of our study is to report the outcomes of patients with BABRA including those with poor grades, underwent endovascular repair.
METHODS: 24 consecutive patients who had endovascular repairs of BABRA from Jan 2011 to Dec 2020 were enrolled. Patient data collected included: demographics, H&H grade, Fisher scale, size of BABRA, and perioperative events. 90- day outcomes were measured using the modified Rankin scale (mRS). Radiographic outcomes were measured using digital subtraction cerebral angiography with Raymond-Roy occlusion classification of intracranial aneurysms.
RESULTS: Twenty-four patients with a median age of 54, underwent endovascular repair of 24 BABRA; median size of 11 mm (4 to 30 mm), wide-neck in 14 patients. Presenting H&H grades was as follows: I in 29%, II in 25%, III in 17% and IV in 29%. 13 patients required external ventricular drain (EVD) and 9 required stent-assisted coiling in acute phase Immediate complete or near complete obliteration achieved in 79% and subtotal in 21%. At 90 days, 75% of patients showed a good outcome (mRS 0 in 14, mRS 1 in 2, mRS 2 in 2) and 25% showed a poor outcome (mRS 3 in 3, mRS 4 in 3, mRS 6 in 1). Of those poor grades H&H IV (7 patients), 57% had good outcomes (mRS 0 in 2, mRS 1 in 2). Recanalization was observed in 9 patients (37%) (1 in small 1, 5 in large & 3 giant), in large and giant aneurysms. Recurrent cases were repaired (5 stent-coil, 4 coiling) without any event and had no impact on their clinical outcomes. There were perioperative complications in 2 patients (one patient developed pontine stroke and achieved mRS 3 and other EVD-related subarachnoid hemorrhage who presented with a H&H of IV, never improved).
CONCLUSION: Endovascular therapy for BABRA is associated with low perioperative risk and good outcomes, including those presented with a poor grade. Endovascular therapy should be considered for all BABRA irrespective of the severity. A high rate of recurrence was observed in large, giant, and partially coiled aneurysms that were repaired and achieved good outcomes. Therefore, all large, giant and partially coiled BABRA warrant an early evaluation for recurrences. Further studies are required to delineate the standard of care for BABRA.
Neuro-Endovascular repair of ruptured basilar artery bifurcation aneurysms including those with poor grades: A single center study
Lodi Y ,Babiker A ,Azab M ,Rosenbaum D
INTRODUCTION
Non-traumatic subarachnoid hemorrhage (SAH) is primarily caused by intracranial aneurysms, which account for 70-80% of all SAH cases. If left untreated, ruptured aneurysms carry a high mortality rate and pose a risk of rebleeding. Therefore, understanding how to diagnose and treat these aneurysms is crucial to maximizing positive clinical outcomes. Identification of the best treatment modality has been a widely researched topic. Microsurgical clipping was the standard of care for treating intracranial aneurysms before 1995. For many years, surgical clipping was considered the gold standard of care for treating intracranial aneurysms, with endovascular coiling being reserved for cases where surgical intervention was deemed too risky. In fact, surgical clipping had been in use for several decades and had a well-established track record of success, with a reported complete occlusion rate of approximately 90% and a low risk of aneurysm recurrence [1, 2]. Numerous studies have shown positive post-operative outcomes in patients that underwent surgical clipping of unruptured and ruptured aneurysms [3, 4]. Most of the outcome data are based on the aneurysms in the anterior circulation, and there is minimum data on the posterior circulation. However, in the early 1990s, endovascular coiling emerged as a new and promising alternative to surgical clipping. Endovascular coiling was shown to be less invasive, with shorter hospital stays and less morbidity with functional outcomes than surgical clipping [5].
The International Subarachnoid Aneurysm Trial (ISAT), a landmark study published in 2005, that compared the outcomes of endovascular coiling versus surgical clipping in patients with ruptured intracranial aneurysms. The study found that endovascular coiling was associated with a significantly better clinical outcome, including lower mortality and fewer cases of severe disability than surgical clipping. Additionally, coiling was associated with higher rates of seizure-free survival [6]. Follow up studies of cohort confirmed that patients who received endovascular repair had better chances of long-term survival and independence compared to those who underwent clipping. Furthermore, the coiling group continued to have better death-free survival and independence despite a higher incidence of aneurysm recurrence and rupture. However, the ISAT study was primarily composed of patients with anterior circulation aneurysms that had good initial clinical presentations. The results could not be applied to patients with posterior circulation aneurysms, larger and complex aneurysms, and those with poor grades on presentation. The Barrow Ruptured Aneurysm Trial (BRAT) compared the outcomes of endovascular coiling versus surgical clipping in patients with ruptured aneurysms. The BRAT found that endovascular coiling was associated with a higher rate of incomplete aneurysm occlusion and higher rates of rebleeding compared to surgical clipping [7]. However, endovascular coiling was associated with better functional outcomes at one year, particularly in patients with poor-grade subarachnoid hemorrhage. The study concluded that both treatment modalities can be effective in the treatment of anterior circulation aneurysms, and that the choice of treatment should be based on individual patient characteristics and preferences.
The results of these studies significantly impacted the management of anterior circulation aneurysms. Since the publication of these studies, the institutional management of anterior circulation aneurysms has shifted towards endovascular coiling with stent-coiling and flow diversion particularly for smaller aneurysms that are easily accessible in the deep critical areas of cerebral circulations. The management of posterior circulation aneurysms was not impacted dramatically. As more studies began to show good clinical outcomes, endovascular coiling became the first line treatment for posterior circulation aneurysms as well [8, 9]. However, there are still questions about how to approach these aneurysms for multiple factors, such as aneurysm size, location, and patient's age, presenting grades and especially, those with poor grades. Presenting H&H grades is considered an excellent predictor of outcomes in the anterior circulation, and poor grades are associated with 75% of mortality and morbidity. However, many patients presenting poor grades can be related to hydrocephalus and mass effects. Due to the anatomic location of the posterior circulation, a small hydrocephalus or mass effect may significantly impair consciousness, leading to the manifestation of poor grades in BABRA. Additionally, there is limited data on poor grade presentations and outcomes in posterior circulation ruptured aneurysms.
Basilar artery bifurcation ruptured aneurysm (BABRA) is a posterior circulation aneurysm accounting for 5-8% of all aneurysms [10]. They are difficult to treat surgically for numerous reasons: the difficulty of open surgical access, the proximity of crucial structures around the interpeduncular fossa like thalamic perforator arteries, nearby cranial nerves, the wide neck of the aneurysm, high rate of recurrence, and risk of retraction injuries. Morbidity and mortality have been shown to be between 28.0-47.4% in patients who underwent surgical repair of BABRA [11] and related to the complex anatomy with presence of unavoidable perforators (Figure 1a & 1b). However, these aneurysms can be safely treated with an endovascular approach, with or without stent use. Success rates from 73-96% have been demonstrated [12- 15]. BABRAs are prone to rupturing as they grow, leading to subarachnoid hemorrhage. Studies have shown a risk of 15% over 7.5 years in aneurysms that measured 10 to 24 mm in diameter. To compare, the risk of rupture for aneurysms in these locations that measured less than 10 mm was approximately 2.5% over 7.5 years [16]. Furthermore, the ISUIA study identified that posterior circulation aneurysms, including BABRA s, were more likely to rupture than those arising from anterior circulation [17]. BABRAs have a mortality rate as high as 23% [18].
There is currently no consensus on how to approach patients with ruptured BABRA who initially present with poor H&H grades (IV-V), and whether they would benefit from intervention. This is due to a paucity of literature on outcomes and complications in patients with ruptured basilar artery aneurysms that initially presented with poor H&H grades. This is the hypothesis of author based on the experiences, most common causes of presenting poor grades are due to the development of acute hydrocephalus and distribution of blood in a very small posterior fossa. Therefore, initial stabilization with ABC and placement of an extra-ventricular catheter placement (EVD) may lead to improved H&H grades and become a candidate for repair of the aneurysm, and potential chance of survival. Vallee et al. 2003 concluded that endovascular treatment with detachable coils is a safe and effective option for treating basilar tip aneurysms, particularly in patients who are not suitable for surgical treatment [11]. This study found that immediate treatment success was predicted by factors such as aneurysm size and neck width. Additionally, factors such as patient age and aneurysm location influenced long-term outcomes. While BABRA were adequately represented in proportion of the aneurysms examined (41/55), only 2 presented with a poor H&H grade (IV). More data is required on perioperative complications and long-term clinical outcomes in patients with severe H&H grades so that management of these aneurysms can be shaped to maximize results in patients. This study aims to address the deficiency in literature. In this study, we present a patient population that all presented with BABRA (including poor grades) that underwent ET with the goal of examining postoperative outcomes.
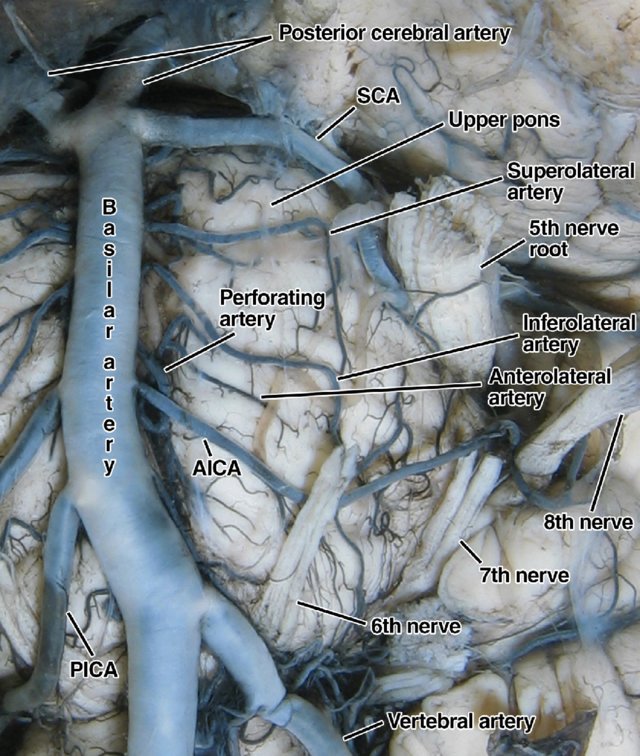
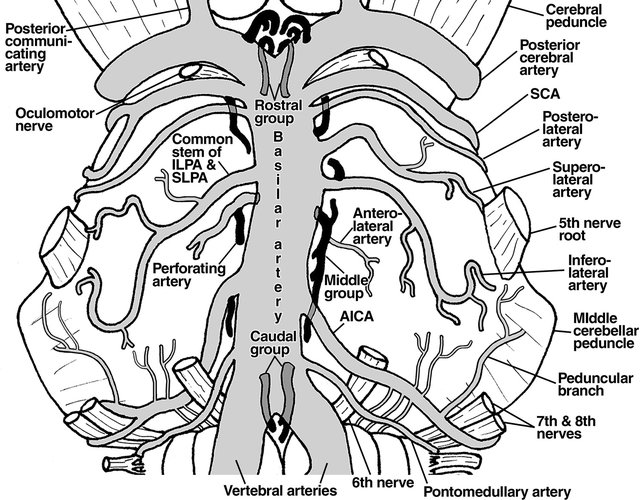
Figure 1a and 1b. A dissection showing the complex anatomy surrounding the basilar artery and a corresponding schematic (Vlaskovic, Brkic [19]
METHODS
In this retrospective study, we systematically analyzed data from a series of patients who underwent endovascular intervention for basilar artery bifurcation ruptured aneurysms (BABRA) during a six-year period, from January 2011 to December 2020. The Hunt & Hess (H&H) grading system, Fisher scale, aneurysm dimensions, and perioperative events were meticulously recorded for each subject. The primary outcome measure for the 90-day follow-up was the modified Rankin scale (mRS), while radiographic outcomes were assessed using digital subtraction cerebral angiography in conjunction with the Raymond-Roy occlusion classification for intracranial aneurysms.
Standard subarachnoid hemorrhage (SAH) management protocols were employed to stabilize patients within the cohort. Specifically, individuals with an H&H grade of 3B or higher were subjected to intubation. A comprehensive evaluation of the technical aspects of the endovascular repair, intraoperative imaging, and patient outcomes was performed, employing mRS, National Institutes of Health stroke scale (NIHSS), or Glasgow Outcome Scale (GOS) as appropriate.
For those patients who underwent stent-assisted coiling, a six-hour preparation period with EVD was followed by a repeated computed tomography (CT) scan to monitor EVD track hemorrhagic and SAH progression. All procedure was performed under general anesthesia via Trans-femoral approach and a systolic blood pressure more than 100 and less than 140 mm Hg was maintained until the aneurysm was repaired. The guiding catheter was continuously flushed with double heparin (4000 units of heparin in 1000 ml normal saline) and nitroglycerine (1 mg of nitroglycerine was added to heparinized saline). First, a diagnostic cerebral angiography and decision of neuro-endovascular approach were made. First, a SL 10 microcatheter was placed on the parent artery covering the neck of the aneurysm, and a second SL 10 microcatheter was navigated close to the aneurysm. At this time a crushed loading dose of 324 mg aspirin(chewable) and 300 mg clopidogrel was administered via nasogastric (NG) tube. A 45- to
60-minute interval was then observed before stent deployment. Most cases a few coils were deployed prior to the deployment of the stent. Intravenous heparin was administered after the deployment of the 2nd coils/when dome was secured. Postoperative management included vigilant monitoring cerebral vasospasm and continuation of antiplatelets for those who received stent. For the primary coiling authors used a similar technique except no antiplatelets was administered before the procedure. No balloons were used in this series. We maintained serum sodium levels within the range of 140-150 mmol/L and close monitoring of intake and output balances of fluids was performed.
RESULTS
The present study encompasses a cohort of 24 patients, aged between 31 and 71 years (median age: 54), who underwent endovascular repair for basilar artery aneurysms. The cohort comprised 19 females and 5 males, with 20 patients identified as active smokers and diagnosed with hypertension. Immediate endotracheal intubation required in 11 patients and an extraventricular drainage (EVD) was placed in 13 patients. Aneurysm dimensions ranged from 4 to 30 mm, with a median size of 11 mm. Wide-neck aneurysms were identified in 14 patients, and all 24 patients presented with ruptured aneurysms. The distribution of patients according to their H&H grades was as follows: 29% with grade I, 25% with grade II, 17% with grade III, and 29% with grade IV (Figure 2).
Of the total patient population, 15 individuals underwent primary coiling (Fig 3A, 4A) while 9 received stentassisted coiling. Immediate and near-total aneurysm obliteration was achieved in 79% of patients, whereas subtotal resolution was observed in 21%. Regarding outcomes, 90-day good outcomes were documented in 75% of patients; 14 patients achieved mRS 0, 2 patients with mRS 1, and 2 patients with mRS 2. Among the 7 patients with H&H grade IV, 57% exhibited good outcomes, with mRS 0 in 2 patients and mRS 1 in 2 patients. Two patients experienced perioperative complications: one developed a pontine stroke and subsequently achieved an mRS 4, while the other, initially presenting with an H&H grade IV, experienced EVD-related subdural hemorrhage, patient never improved from the initial presentation and died.
Aneurysm recanalization developed in 9 patients (1 small, 5large, and 3 giant) mostly in large and giant aneurysms including those achieved subtotal obliteration. Recurrences were observed for 3-6 months of follow-up angiographic evaluations. Recurrent cases were repaired; 5 with stent assisted coiling (Figure 4B) and 4 with coiling (Figure 3B) and had no impact on their functional outcomes.
Table 1: Clinical Outcomes and Follow-Up Data for Endovascular Repair of Ruptured BABRA
|
Parameter |
Value |
|
Total Patients |
24 |
|
Age (Range, Median) |
31–71 years (Median: 54) |
|
Gender |
Female: 19 (79%), Male: 5 (21%) |
|
Risk Factors |
Hypertension: 20 (83%), Active Smokers: 20 |
|
Hunt & Hess Grade |
I: 6 (29%), II: 4 (25%), III: 4 (17%), IV: 6 (29%) |
|
Aneurysm Size |
Range: 4–30 mm (Median: 11 mm) |
|
Wide-Neck Aneurysms |
14 patients |
|
Treatment Type |
Primary Coiling: 15 (62%), Stent-Assisted Coiling: 9 (38%) |
|
Immediate Occlusion |
Complete/Near Complete: 79%, Subtotal: 21% |
|
90-Day Outcomes (mRS) |
Good (0–2): 18 (75%), Poor (≥3): 6 (25%) |
|
Grade IV Outcomes |
Good: 4/7 (57%) |
|
Perioperative Complications |
Pontine Stroke: 1 (mRS 4), EVD-related SAH: 1 (Death) |
|
Follow-Up Period |
3–12 months |
|
Recurrence Observed |
9 patients (37%) |
|
Aneurysm Size in Recurrence |
Small: 1, Large: 5, Giant: 3 |
|
Timing of Recurrence |
3–6 months post-procedure |
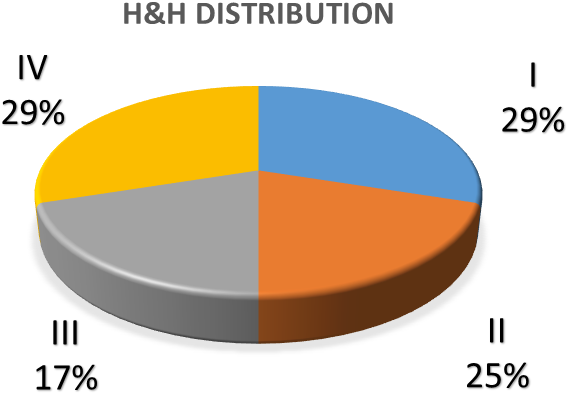
Figure 2: Hunt and Hess graphic distributions

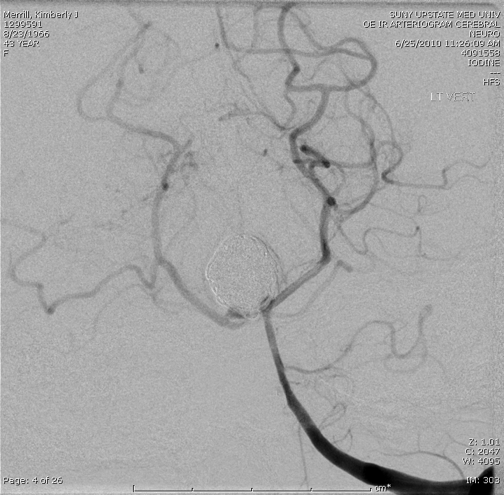
Figure 3A: 41 Y/O women with history uncontrolled blood pressure and smoking presented with SAH with H&H of I due to the ruptured basilar artery complex aneurysm underwent repair with small residual who required subsequent coiling

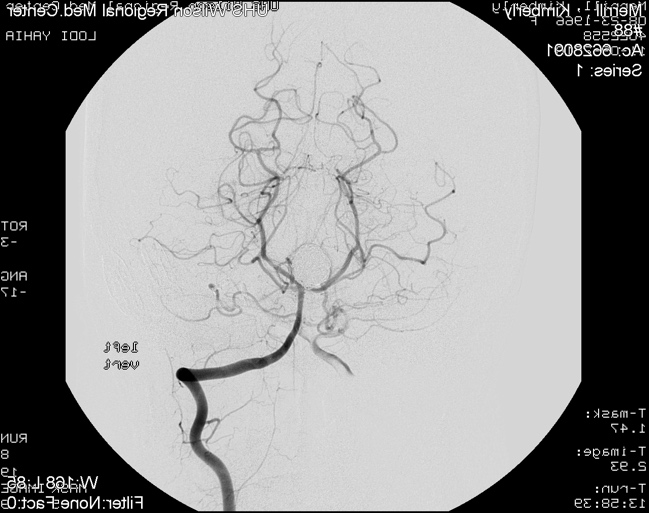
Figure 3B: Residual aneurysm was repaired. 1-year follow-up revealed persistence obliteration

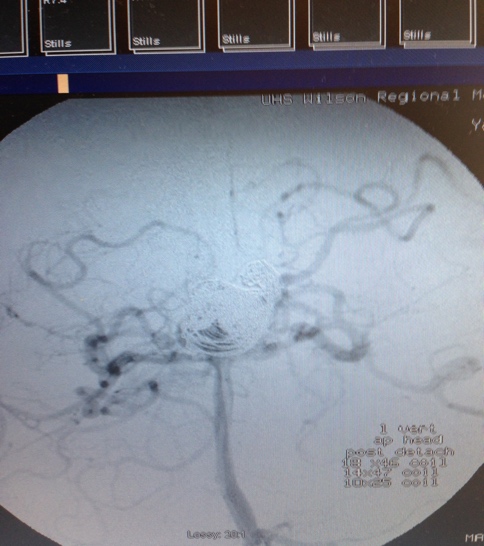
Figure 4A: 58 Y/O man underwent primary endovascular coiling of a giant ruptured BA aneurysm

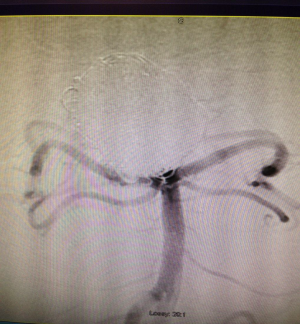
Figure 4B: 6 months follow-up angiogram demonstrated recurrence resulted in Y stent-assisted repair.
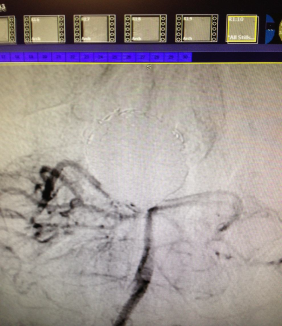
Figure 4C: Persistence obliteration in 12 months follow-up cerebral angiography 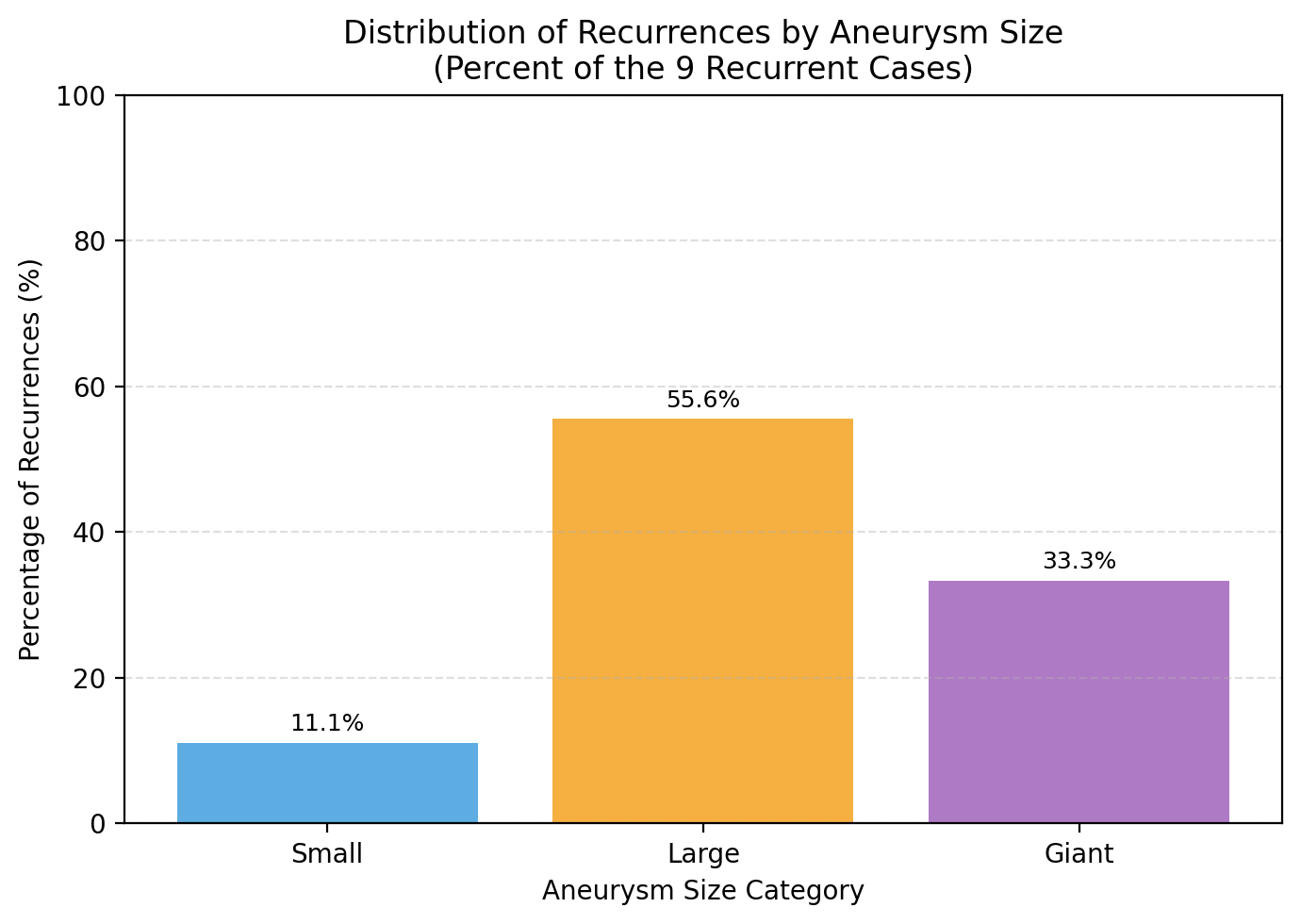 Figure 5. Shows the composition of recurrences by size among the 9 recurrent cases.
Figure 5. Shows the composition of recurrences by size among the 9 recurrent cases.
DISCUSSION
Although the natural history of BABRA is not completely known, there are multiple factors that contribute to its higher risk of rupturing if left untreated compared to other intracerebral aneurysms. Kolk et al 2010 propose that BABRA embryologic origins, bifurcation anatomy, hemodynamic, vascular structural changes, and local environment all play large roles in aneurysm formation and fragility [20]. Ho et al. demonstrated that another predictor is the angle of the posterior communicating artery [21]. Individuals with a ruptured BABRA were found to have a significantly greater angle of the PCA than those with an intact BABRA. Another retrospective study has demonstrated that the presence of a daughter dome, higher aspect ratios, and larger flow angles were significantly linked to basilar aneurysm rupture status. Furthermore, multilobed aneurysms were found to be associated with a higher risk of rupture compared to nonmultilobed aneurysms. Additionally, a smaller basilar artery diameter, relative to the posterior cerebral arteries, was believed to contribute to higher jet flow at the basilar apex, leading to increased hemodynamic stress, structural fatigue, and eventual rupture [22]. In short, although BABRA are rare, they carry a significant risk of rupture that is highly dependent on multiple variables.
Our study aimed to assess the clinical outcomes and perioperative complications, including those who initially presented with poor H&H grades (IV-V) and underwent endovascular repair. In our cohort of 24 patients, 29% presented with H&H grade IV, emphasizing the importance of understanding the treatment outcomes for this patient population. Endovascular treatment has become the preferred method of intervention for intracranial aneurysms, especially in the anterior circulation, due to the less invasive nature of the procedure and the better clinical outcomes reported in landmark studies such as the International Subarachnoid Aneurysm Trial (ISAT). Multiple studies have since advocated for use of endovascular therapy for posterior circulation aneurysms [2, 23-25]. However, the literature regarding poor grade ruptured posterior circulation aneurysms, including BABRA, is still limited, and the optimal treatment strategy for this is yet to be determined. The management of BABRA is particularly challenging due to the complex anatomy of the region, the proximity of critical neurovascular structures, and the increased risk of rupture and rebleeding associated with these aneurysms. In our study, we found that endovascular treatment, either with primary coiling or stent-assisted coiling, resulted in immediate and near complete obliteration of the aneurysm in 79% of patients and subtotal resolution in 21% of the patients. The 90-day outcomes were good in 75% of the patients, with mRS 0 in 14 patients, mRS 1 in 2 patients, and mRS 2 in 2 patients. This indicates that endovascular repair can be a viable treatment option for patients with BABRA, even in those with poor initial clinical presentation.
When specifically examining the outcomes of patients who presented with H&H grade IV, we found that positive` outcomes were recorded in 57%, with mRS 0 in 2 patients and mRS 1 in 2 patients. Although this rate is lower than the overall positive outcome rate in our cohort, it demonstrates that endovascular treatment may still be beneficial for patients with poor-grade subarachnoid hemorrhage caused by BABRA. Additionally, our study found that aneurysm recanalization was required in 9 patients, including those with subtotal obliterated cases. Both unruptured and ruptured basilar artery aneurysms have a high rate of recurrence and progression [26]. A considerable aneurysm recurrence rate was noticed in our study, especially in large, giant, and partially coiled aneurysms. This necessitated early assessments for certain patients prior to their scheduled 90-day follow up. However, no influence on outcomes was observed in those requiring recanalization. BABRA morphology and location increase coil compaction risk, with complete coil obliteration only filling 30% of the aneurysm [27]. A 90%-100% occlusion can protect against hemorrhage, while 50%-90% occlusion helps in ruptured aneurysms [28]. Smaller-neck aneurysms are easier to occlude, but wider-necked aneurysms (>4 mm) have a higher recanalization risk and need close monitoring due to flow dynamics and stress [29]. Prior studies have shown that this is not an uncommon outcome in patients with unruptured basilar artery bifurcation aneurysms or ruptured BABRA with good initial H&H grades [28, 30, 31]. Therefore, long-term durability of endovascular repair may require further investigation.
Perioperative complications were observed in 2 patients: one patient developed a pontine stroke after primary coiling, and another patient who had an initial H&H grade IV developed EVD-related subdural hemorrhage who never recovered from grade IV and ultimately died. Hydrocephalus was the most common finding observed in our study after SAH, with 13 out of 24 patients requiring placement of an EVD. It is the hypothesis of the authors that addressed immediately which led to the improvement of the H&H grades after presentation, and may be responsible for the outcomes, especially those presented with poor grades. Nam et al 2010 has shown that it has a higher incidence in poor-grade aneurysms treated with coiling, which is consistent with our study [32]. These findings highlight the importance of careful patient selection, individualized treatment planning, and meticulous perioperative management to minimize complications and optimize outcomes.
The limitations of our study include its retrospective design and the relatively small sample size, which may limit the generalizability of our findings. Moreover, our study lacks a control group of patients who underwent microsurgical clipping or conservative management, making it difficult to draw definitive conclusions about the superiority of endovascular treatment. Nevertheless, our study provides valuable insights into the clinical outcomes of endovascular repair in patients with BABRA and poor H&H grades, contributing to the growing body of evidence supporting the use of endovascular treatment for this challenging patient population. In conclusion, our study demonstrates that endovascular repair can be a feasible and effective treatment option for patients with BABRA, including those with poor initial clinical presentation. While our findings suggest that endovascular treatment may lead to positive outcomes in a majority of patients, further research is needed to determine the optimal treatment strategy for patients with BABRA in the posterior circulation.
CONCLUSION
This study demonstrates that endovascular repair s an effective treatment for patients with basilar artery bifurcation ruptured aneurysms (BABRA), including those presenting with severe Hunt and Hess (H&H) grades, with positive 90-day outcomes in 75% of the patients. Although positive outcomes were lower in patients with H&H grade IV, Notably, 57% of patients with grade IV achieved good recovery, supporting the role of endovascular therapy even in severe clinical presentations. Perioperative complications were observed in some cases, emphasizing the need for careful patient selection, individualized treatment planning, and meticulous perioperative management. Aneurysm recanalization was required in several patients, indicating that the long-term durability of endovascular repair for ruptured BABRA may need further investigation. Limitations of the study include its retrospective design, small sample size, and lack of a control group. Despite these constraints, the findings add to the growing evidence supporting endovascular treatment for ruptured BABRA in patients with poor grades. Future prospective studies with larger cohorts and comparative arms are needed to establish optimal treatment strategies and assess longterm outcomes relative to alternatives such as microsurgical clipping or conservative management.
1. Bederson, J.B., et al., Recommendations for the management of patients with unruptured intracranial aneurysms: A statement for healthcare professionals from the Stroke Council of the American Heart Association. Circulation, 2000. 102(18): p. 2300-8.
2. Wiebers, D.O., et al., Unruptured intracranial aneurysms: natural history, clinical outcome, and risks of surgical and endovascular treatment. Lancet, 2003. 362(9378): p. 103-10.
3. Meyer, F.B., et al., Medical and surgical management of intracranial aneurysms. Mayo Clin Proc, 1995. 70(2): p. 153-72.
4. Solomon, R.A., M.E. Fink, and J. Pile-Spellman, Surgical management of unruptured intracranial aneurysms. Journal of Neurosurgery, 1994. 80(3): p. 440- 446.
5. Brilstra, E.H., et al., Treatment of intracranial aneurysms by embolization with coils: a systematic review. Stroke, 1999. 30(2): p. 470-6.
6. Molyneux, A.J., et al., International subarachnoid aneurysm trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms: a randomised comparison of effects on survival, dependency, seizures, rebleeding, subgroups, and aneurysm occlusion. Lancet, 2005. 366(9488): p. 809-17.
7. McDougall, C.G., et al., The Barrow Ruptured Aneurysm Trial. J Neurosurg, 2012. 116(1): p. 135-44.
8. Lempert, T.E., et al., Endovascular treatment of ruptured posterior circulation cerebral aneurysms. Clinical and angiographic outcomes. Stroke, 2000. 31(1): p. 100-10.
9. Tsianaka, E., et al., Clipping versus coiling in posterior circulation intracranial aneurysms: a meta-analysis. Chin Neurosurg J, 2019. 5: p. 16.
10. Spiessberger, A., et al., Microsurgical Clipping of Basilar Apex Aneurysms: A Systematic Historical Review of Approaches and their Results. World Neurosurg, 2018. 114: p. 305-316.
11. Vallee, J.N., et al., Endovascular treatment of basilar tip aneurysms with Guglielmi detachable coils: predictors of immediate and long-term results with multivariate analysis 6-year experience. Radiology, 2003. 226(3): p. 867-79.
12. Chalouhi, N., et al., Safety and efficacy of endovascular treatment of basilar tip aneurysms by coiling with and without stent assistance: a review of 235 cases. Neurosurgery, 2012. 71(4): p. 785-94.
13. Peluso, J.P., et al., Coiling of basilar tip aneurysms: results in 154 consecutive patients with emphasis on recurrent haemorrhage and re-treatment during mid- and long-term follow-up. J Neurol Neurosurg Psychiatry, 2008. 79(6): p. 706-11.
14. Sato, E., et al., Applications and Roles of Coil Embolization and/or Clipping in the Treatment of Cerebral Aneurysm. Interv Neuroradiol, 2006. 12(Suppl 1): p. 77-85.
15. Tjahjadi, M., J. Serrone, and J. Hernesniemi, Should we still consider clips for basilar apex aneurysms? A critical appraisal of the literature. Surg Neurol Int, 2018. 9: p. 44.
16. Morey, S.S., AHA recommendations for the management of intracranial aneurysms. Agency for Health Care Policy and Research. Am Fam Physician, 2001. 63(12): p. 2465-6.
17. Raymond, J., et al., Unruptured Intracranial Aneurysms. A Critical Review of the International Study of Unruptured Intracranial Aneurysms (ISUIA) and of Appropriate Methods to Address the Clinical Problem. Interv Neuroradiol, 2008. 14(1): p. 85-96.
18. Ge, H., et al., The role of endovascular treatment in unruptured basilar tip aneurysms. Interv Neuroradiol, 2017. 23(1): p. 8-13.
19. Vlaskovic, T., et al., Anatomic and MRI Bases for Pontine Infarctions with Patients Presentation. J Stroke Cerebrovasc Dis, 2022. 31(8): p. 106613.
20. van der Kolk, N.M., A. Algra, and G.J. Rinkel, Risk of aneurysm rupture at intracranial arterial bifurcations. Cerebrovasc Dis, 2010. 30(1): p. 29-35.
21. Ho, A.L., A. Mouminah, and R. Du, Posterior cerebral artery angle and the rupture of basilar tip aneurysms. PLoS One, 2014. 9(10): p. e110946.
22. Zhang, J., et al., Morphological variables associated with ruptured basilar tip aneurysms. Scientific Reports, 2021. 11(1): p. 2526.
23. Lanzino, G., et al., Coil embolization versus clipping for ruptured intracranial aneurysms: a meta-analysis of prospective controlled published studies. AJNR Am J Neuroradiol, 2013. 34(9): p. 1764-8.
24. Li, H., et al., Clipping versus coiling for ruptured intracranial aneurysms: a systematic review and metaanalysis. Stroke, 2013. 44(1): p. 29-37.
25. Winkler, E.A., et al., Endovascular embolization versus surgical clipping in a single surgeon series of basilar artery aneurysms: a complementary approach in the endovascular era. Acta Neurochir (Wien), 2021. 163(5): p. 1527-1540.
26. Ge, H., et al., Endovascular Treatment of Large or Giant Basilar Artery Aneurysms Using the Pipeline Embolization Device: Complications and Outcomes. Front Neurol, 2022. 13: p. 843839.
27. Kawanabe, Y., et al., Endovascular occlusion of intracranial aneurysms with Guglielmi detachable coils: correlation between coil packing density and coil compaction. Acta Neurochir (Wien), 2001. 143(5): p. 451-5.
28. Henkes, H., et al., Endovascular coil occlusion of 1811 intracranial aneurysms: early angiographic and clinical results. Neurosurgery, 2004. 54(2): p. 268-80; discussion 280-5.
29. Henkes, H., et al., Angiographic and clinical results in 316 coil-treated basilar artery bifurcation aneurysms. J Neurosurg, 2005. 103(6): p. 990-9.
30. Lozier, A.P., et al., Guglielmi Detachable Coil Embolization of Posterior Circulation Aneurysms. Stroke, 2002. 33(10): p. 2509-2518.
31. McDougall, C.G., et al., Endovascular treatment of basilar tip aneurysms using electrolytically detachable coils. J Neurosurg, 1996. 84(3): p. 393-9.
32. Nam, K.H., et al., Risk of Shunt Dependent Hydrocephalus after Treatment of Ruptured Intracranial Aneurysms : Surgical Clipping versus Endovascular Coiling According to Fisher Grading System. J Korean Neurosurg Soc, 2010. 48(4): p. 313-8.