Evaluating the Impact of Phlebotomy Training and Staffing Adjustments on Blood Culture Contamination in an Academic Medical Center
Farzana Hoque ,Lori Hainaut ,Nongnooch Poowanawittayakom
1Associate Professor of Medicine, Saint Louis University School of Medicine, St. Louis, MO, USA
2SSM Health Saint Louis University Hospital, St. Louis, MO, USA
3Assistant Professor of Medicine, Washington University in St. Louis, MO, USA
Background: Blood culture contamination remains a persistent quality and patient safety challenge, particularly in emergency departments (EDs), where operational pressures may compromise sterile techniques. Accepted contamination benchmarks are <3%, with institutional targets often set lower. Contamination increases unnecessary antibiotic exposure, length of stay, and healthcare costs.
Objective: To evaluate the impact of two sequential quality improvement (QI) interventions focused on standardized phlebotomy technique on blood culture contamination rates across a tertiary care hospital.
Methods: Two blood culture collection interventions were implemented at a university-affiliated tertiary hospital. The first was a house-wide phlebotomystandardization initiative (June 2021), including ED, four ICUs, and inpatient medical and surgical units. The second was an ED-specific intervention (April 2022) limiting collection to selected specially trained nurses. Contamination data were collected 6 months before and after the house-wideintervention and 15 months before and 6 months after the ED intervention. Mean contamination rates were compared using two-sided ttests.
Results: A total of 24,361 blood cultures were analyzed (12,951 pre-intervention; 11,410 post-intervention). Prior to implementation, mean contamination rates were 2.31% house-wide and 4.43% in the ED. After implementation, mean contamination rates were 3.11% house-wide and 4.83% in the ED. The absolute difference in house-wide contamination rate was +0.80 percentage points (95% CI, −1.83% to +3.43%). The absolute difference in ED contamination rate was +0.40 percentage points (95% CI, −4.65% to +5.45%). Two-sided t-testing yielded p = 0.537, indicating no statistically significant difference.
Conclusions: Standardization of phlebotomy technique alone did not significantly reduce contamination rates. Multifaceted strategies targeting workflow, accountability, and process adherence may be required to achieve sustained improvement below national benchmarks
Keyword: Blood culture contamination Emergency department Intervention
Evaluating the Impact of Phlebotomy Training and Staffing Adjustments on Blood Culture Contamination in an Academic Medical Center
Farzana Hoque ,Lori Hainaut ,Nongnooch Poowanawittayakom
1Associate Professor of Medicine, Saint Louis University School of Medicine, St. Louis, MO, USA
2SSM Health Saint Louis University Hospital, St. Louis, MO, USA
3Assistant Professor of Medicine, Washington University in St. Louis, MO, USA
INTRODUCTION
Blood culture contamination is a persistent, nationwide quality problem, particularly in emergency departments (EDs) where high patient volume, staff turnover, and time pressure to obtain cultures before antibiotic administration can compromise collection technique.1,2 The Clinical and Laboratory Standards Institute (CLSI) benchmark for acceptable blood culture contamination is <3%.1,2 Our institutional goal is more stringent (<2%), reflecting the clinical and operational burden of falsepositive results.1,8 Most blood culture contaminants are skin flora, emphasizing that meticulous skin antisepsis and standardized sterile technique are central to prevention.3,6 Interventions that improve sterile technique—including optimized skin antisepsis, standardized kits, procedural checklists, and sterile gloving—have been associated with meaningful reductions in contamination.3,6,7 In a large interrupted time-series quality improvement study, converting ED collection from a “clean” approach to a standardized sterile approach significantly reduced contamination and sustained performance below the 3% benchmark.7 Collection source and technique also affect contamination. Cultures drawn from central venous catheters can increase false positives from line colonization or luminal contamination, and guidelines and institutional practices often favor peripheral venipuncture when feasible.4 The volume of blood cultured remains a key determinant of diagnostic yield; inadequate volume reduces organism recovery and may prompt repeat cultures and additional downstream testing.5 Per manufacturer and laboratory guidance, our standard adult practice is to inoculate each bottle with 8–10 mL of blood.5 Blood culture contamination has significant downstream consequences for patients and health systems, including unnecessary antibiotic exposure, additional diagnostic testing, longer hospital stays, avoidable procedures (including line removal), and increased costs.6,8 Beyond contamination, overordering of blood cultures in low-yield scenarios compounds these harms: low diagnostic yield in hospitalized medical patients has been described, with a substantial proportion of cultures drawn for isolated fever or leukocytosis without bacteremia.10
Diagnostic stewardship interventions can safely reduce unnecessary blood culture utilization without worsening key safety outcomes, reinforcing that “right test, right patient, right time” is a complementary target alongside contamination reduction.9,12 Additionally, unnecessary blood cultures contribute to patient suffering in ways that are often under-measured: repeated venipuncture can drive patient frustration, disrupt rest, and increase the cumulative volume of phlebotomy-associated blood loss.11 In critically ill adults, contemporary data demonstrate substantial cumulative phlebotomy volumes during hospitalization with associations between higher blood loss, lower nadir hemoglobin, increased transfusion, and significant institutional cost burden.11 Quality improvement efforts that reduce contamination and reduce unnecessary ordering can therefore address patientcentered outcomes while also improving antimicrobial stewardship and lowering avoidable costs.6,8,9,11,12
Our initial evaluation demonstrated that the blood culture contamination rate was significantly lower in cultures collected by phlebotomists compared with nurse-collected cultures. Based on this observed gap, we implemented a phlebotomy-standard technique across the ED, intensive care units (ICUs), and inpatient units, training nursing staff in phlebotomy-standard collection and monitoring performance over time. A second intervention followed in the ED, in which a smaller, dedicated subset of trained nurses performed phlebotomy-standard blood culture collection
METHODS
Study Setting and Interventions
This quality improvement (QI) project was conducted at a single university-affiliated tertiary care hospital in the United States. The interventions included:
1. House-wide standardization (June 2021): Focused phlebotomy training for nursing staff across the ED, four ICUs, and ten inpatient floors.
2. ED-specific intervention (April 2022): Limiting blood culture collection in the ED to a smaller, dedicated subset of specially trained nurses.
Definition of Contamination
A blood culture set was defined as cultures obtained from a single blood draw (1 or 2 bottles). A set was classified as contaminated when an organism from the microbiology laboratory’s “possible contaminant” list was isolated in <50% of all sets obtained from the same patient on the same date, using laboratory adjudication rules:
1. Contaminant if it was the only blood culture collected.
2. Contaminant if cultures drawn within 48 hours were negative or grew a different organism.
3. Not a contaminant if cultures drawn within 48 hours grew the same organism.
4. Cultures with the same documented collection time (within 3 minutes) were not treated as separate cultures
Statistical Analysis
Data was collected 6 months pre/post house-wide implementation and 15 months pre/6 months post ED intervention. Mean contamination rates were compared using two-sided t-tests, with significance defined as p < 0.05.
RESULTS
A total of 12,951 blood cultures were collected before implementation. After both interventions, 11,410 blood cultures were collected, resulting in a total of 24,361 blood cultures being analyzed. The Emergency Department (ED) collected the highest number of blood cultures in both the pre- and post-intervention periods, whereas the psychiatry inpatient units performed the lowest number of blood cultures. Before the house-wide and ED-specific interventions, the mean contamination rates were 2.314% and 4.43%, respectively. After implementation, the mean contamination rates were 3.109% house-wide and 4.83% in the ED (Table 1). A two-sided t-test yielded a p-value of 0.537, which exceeded the predefined threshold for statistical significance (p < 0.05). Consequently, no statistically significant difference in contamination rates was observed following the implementation of the standardized training program (Figure 1).
Mean contamination rates demonstrated significant heterogeneity across clinical environments, ranging from 0% to 16.67% across units and time periods (Table 2). While psychiatry inpatient units maintained the lowest mean contamination rate (0%), the highest mean rates were consistently observed in high-acuity areas. This wide variance underscores the departmental heterogeneity within the tertiary center and suggests that units with higher clinical acuity and rapid turnover present unique challenges to maintaining sterile collection protocols (Table 2).
Table 1. Core Results by Setting
|
Setting |
Pre-Intervention Rate (%) |
Post-Intervention Rate (%) |
Absolute Change |
|
House-wide |
2.31% |
3.1% |
+0.80% |
|
Emergency Department |
4.43% |
4.83% |
+ 0.40% |
Table 1 Note. Comparison of mean blood culture contamination rates before and after implementation of standardized phlebotomy training and ED-specific staffing adjustments. House-wide data represent a 6-month pre/post-intervention period. ED data reflect a 15-month pre-intervention and 6-month post-intervention period. Differences between periods were not statistically significant (p = 0.537).
Table 2. Blood Culture Contamination Variance by Hospital Unit Type
|
Unit Type |
Volume Category |
Contamination Range (Mean %) |
Significance for Targeted Intervention |
|
Emergency Department |
Very High |
4.43% – 4.83% |
Highest Risk: Requires specialized staffing and kits. |
|
Intensive Care Units (4) |
High |
1.50% – 3.20% |
Moderate Risk: Impacted by acute sepsis protocols. |
|
Inpatient Med/Surg (10) |
Moderate |
1.10% – 16.67% |
High Variance: Likely driven by individual staff technique. |
|
Psychiatry Units |
Low |
0.00% |
Lowest Risk: Low volume and stable environment. |
Estimated based on departmental mean and reported institutional range.
Table 2 Note: Distribution of mean blood culture contamination rates across 15 hospital units. The wide variance (0% to 16.67%) highlights the departmental heterogeneity in a tertiary academic center. Units with higher clinical acuity and rapid turnover, such as the Emergency Department, consistently exhibited higher baseline and post-intervention contamination rates compared to low-volume specialty units.
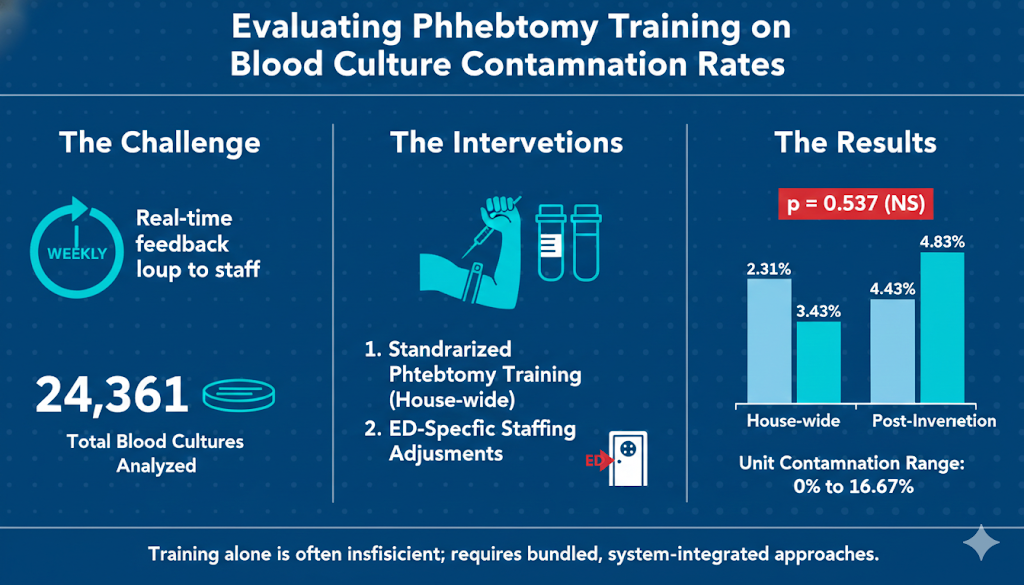
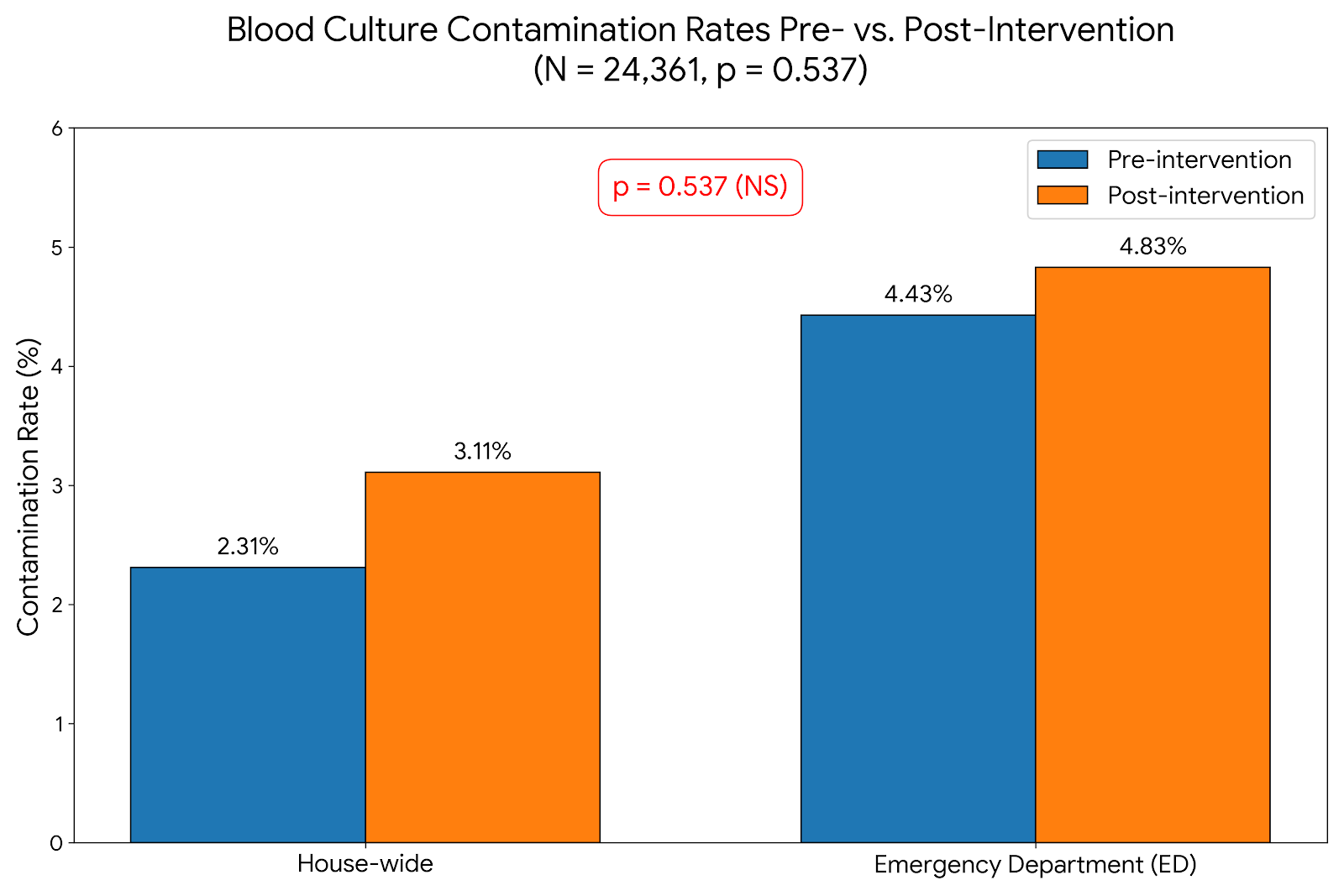
Figure 1. Comparison of Blood Culture Contamination Rates Before and After Multi-Level Quality Improvement Interventions.
Mean contamination rates across the institution ("House-wide") and within the Emergency Department (ED) are presented. The analysis included a total of 24,361 blood cultures (12,951 pre-intervention; 11,410 post-intervention). Standardized phlebotomy training and targeted staffing adjustments did not lead to a statistically significant reduction in contamination rates in either setting (p = 0.537). Aggregate house-wide contamination rates shifted from 2.31% to 3.11%, while ED-specific rates moved from 4.43% to 4.83%.
DISCUSSION
Blood culture contamination directly influences diagnostic accuracy, antimicrobial decision-making, and healthcare utilization. False-positive cultures frequently prompt unnecessary broad-spectrum antibiotic initiation, repeat blood cultures, and additional laboratory testing.6,8 These downstream effects contribute to prolonged hospitalization and increased healthcare costs.6,8 In addition to contamination, unnecessary blood culture ordering in low-yield clinical scenarios further amplifies these harms. Studies demonstrate low diagnostic yield when cultures are obtained for isolated fever or leukocytosis without hemodynamic instability.9,10 In this retrospective study of hospitalized medical patients, Linsenmeyer et al. found that blood cultures obtained solely for isolated fever (“culture if spikes”) had a low diagnostic yield, with true bacteremia identified in a small minority of cases. The findings suggest that routine blood culture collection for fever without additional clinical indicators has limited utility and may contribute to unnecessary testing and resource utilization.10 Diagnostic stewardship interventions have shown that blood culture utilization can be reduced safely without worsening mortality outcomes.9,11,12 Repeated venipuncture is also not benign; hospitalized patients are exposed to substantial cumulative phlebotomy volumes, and higher cumulative blood loss has been associated with iatrogenic anemia and increased transfusion exposure.11 In an observational cohort study of adults aged ≥18 years conducted at a large academic medical center, anemia was found to be highly prevalent among critically ill patients and frequently exacerbated by phlebotomy-associated blood loss during hospitalization. In adjusted analyses, each additional 100 mL of cumulative phlebotomy volume was associated with a 1.15-fold increase in red blood cell (RBC) units transfused (95% confidence interval [CI], 1.14–1.17; P < .001), demonstrating a significant dose–response relationship between diagnostic blood loss and transfusion requirement. The financial impact was substantial, with estimated annual phlebotomy-related costs exceeding $15 million (approximately $2,500 per admission), underscoring both the clinical and economic consequences of excessive laboratory utilization.11 Therefore, QI initiatives targeting contamination should be paired with strategies aimed at reducing unnecessary ordering.
In this study, standardized phlebotomy training and targeted ED staffing adjustments did not produce a statistically significant reduction in contamination rates. These findings are supported by a robust sample size (N = 24,361), providing significant statistical power and a comprehensive longitudinal view of trends across a diverse tertiary care environment. The implementation of sterile collection techniques has been shown to reduce contamination both in academic and community hospitals.9 Previous studies focusing on blood sample collection technique, such as the employment of a diversion tube, resulted in a 31% reduction in contamination compared to contemporaneous cultures obtained without diversion.12 The incidence of contamination in such studies was not changed with respect to the type of bacteria detected.12 We used clear gloves to collect blood samples. A randomized clinical trial analyzed whether blood-culture collection using sterile gloves reduces the contamination rate when compared to clear gloves; this study found no difference in the contamination rate when blood cultures are collected using a sterile modified or clean technique.13 The high-velocity workflow of the ED presents different challenges than inpatient wards, and the reliance on bedside nursing rather than a dedicated phlebotomy team remains a potential limitation. The ED had the highest number of blood cultures collected, indicating the importance of focused intervention in this unit. In contrast, the psychiatry units had the lowest volume, contributing to the lowest mean contamination rate of 0. The highest mean contamination rate of 16.67% underlines the importance of focused interventions in units with higher rates.
Deliberate, evidence-based laboratory stewardship— including judicious blood culture utilization—is fundamental to patient safety, preventing avoidable harm, false positives, unnecessary antibiotics, and also impact patient experience.14,15 Patient experience directly influences reimbursement through the Centers for Medicare & Medicaid Services (CMS) Hospital ValueBased Purchasing Program, making appropriate test utilization both a clinical and financial imperative.14 In academic hospitals, trainees must be trained early to order tests based on clear clinical indications rather than reflexive thoroughness, as unnecessary testing can negatively affect patient experience and value-based care outcomes.
Our study’s use of weekly data and real-time feedback to nursing leaders and frontline nurses is an exemplary approach that could potentially be adopted in other healthcare institutions. Although the differences did not reach statistical significance, contamination rates increased in both the ED and house-wide settings following implementation of the two-person checklist strategy. Several operational and human factors may explain this counterintuitive finding. First, workflow disruption in the high-acuity ED environment may have contributed. The ED is fast-paced and time-sensitive; introducing a second person into the procedure may have interrupted sterile focus during skin preparation, created delays between antisepsis and venipuncture, or increased rushed steps under time pressure. Even minor breaks in sterile techniques such as re-palpating the site after antiseptic application—can increase contamination risk. Second, diffusion of responsibility may have occurred. With two individuals involved, accountability for maintaining sterility may become less clearly defined, and critical steps such as allowing adequate chlorhexidine drying time may be overlooked. Third, incosnsistent role definition could have introduced variability. Without clearly assigned responsibilities (e.g., who preps, who draws, who verifies), the checklist may become procedural rather than protective, resulting in communication gaps or interruptions during key sterile steps. Checklist fatigue may also have played a role. If the process was perceived as burdensome or poorly integrated into existing workflows, staff may have prioritized checklist completion over strict adherence to aseptic technique. Additionally, the two-person model may have unintentionally increased manipulation of supplies and environmental exposure. More handling and more hands involved in the procedure increase opportunities for contamination. ED-specific operational factors— including higher acuity patients, crowded environments, limited space, and time-sensitive sepsis protocols—may have further compounded these challenges. The intervention may have added procedural complexity without addressing root technical drivers such as site selection, antiseptic technique, or competency validation. Finally, measurement artifact cannot be excluded. Increased surveillance, higher culture volumes, or inclusion of higher-risk patients in the postintervention period may have contributed to the observed increase. These findings suggest that workflow-sensitive interventions in high-acuity environments require careful human factors assessment and role standardization prior to implementation. However, several limitations exist. It is likely that the sample size was not large enough to detect a significant difference across so many diverse units. Next, the "series definition" employed to define contamination may not accurately reflect the true contamination rate.9 Furthermore, a potential explanation could be the learning curve associated with implementing a novel technique, as hospital staff may not have fully internalized the proper technique. Our study suggests that behavioral training alone, without mechanical barriers like diversion devices, may be insufficient to overcome the systemic pressures of a busy academic hospital. Future studies with more comprehensive, multidisciplinary bundled interventions are essential to decrease contamination.
CONCLUSION
Standardized phlebotomy training alone did not significantly reduce blood culture contamination rates in this tertiary care hospital. Because contamination and unnecessary ordering both contribute to avoidable antibiotic exposure, excess cost, patient discomfort, and iatrogenic anemia risk, improvement efforts should address both collection quality and diagnostic stewardship. This study highlights the importance of real-time evaluation of the implementation process, giving feedback to frontline staff, and the importance of monitoring and evaluating contamination rates across different units for essential, targeted interventions. Durable reduction in low-value blood culture use will likely require multifaceted, system-level interventions rather than isolated educational strategies.
1. Clinical and Laboratory Standards Institute. Principles and Procedures for Blood Cultures; Approved Guideline. CLSI document M47-A. Clinical and Laboratory Standards Institute; 2007.
2. Baron EJ, Weinstein MP, Dunne WM Jr, et al. Cumitech 1C, Blood Cultures IV. ASM Press; 2005.
3. Washer LL, Chenoweth C, Kim HW, et al. Blood culture contamination: a randomized trial evaluating the comparative effectiveness of 3 skin antiseptic interventions. Infect Control Hosp Epidemiol. 2013;34(1):15-21.
4. Boyce JM, Nadeau J, Dumigan D, et al. Obtaining blood cultures by venipuncture versus from central lines: impact on blood culture contamination rates and potential effect on central line-associated bloodstream infection reporting. Infect Control Hosp Epidemiol. 2013;34(10):1042-1047.
5. Bouza E, Sousa D, Rodríguez-Créixems M, et al. Is the volume of blood cultured still a significant factor in the diagnosis of bloodstream infections? J Clin Microbiol. 2007;45(9):2765-2769.
6. Doern GV, Carroll KC, Diekema DJ, et al. Practical guidance for clinical microbiology laboratories: a comprehensive update on the problem of blood culture contamination and a discussion of methods for addressing the problem. Clin Microbiol Rev. 2020;33(1):e00009-19.
7. Self WH, Speroff T, McNaughton CD, et al. Reducing blood culture contamination in the emergency department: an interrupted time series quality improvement study. Acad Emerg Med. 2013;20(1):89- 97.
8. Dempsey C, Skoglund E, Muldrew KL, Garey KW. Economic health care costs of blood culture contamination: a systematic review. Am J Infect Control. 2019;47(8):963-967.
9. Fabre V, Klein E, Salinas AB, et al. A diagnostic stewardship intervention to improve blood culture use among adult nonneutropenic inpatients: the DISTRIBUTE study. J Clin Microbiol. 2020;58(12):e01053-20.
10. Linsenmeyer K, Gupta K, Strymish JM, et al. Culture if spikes? Indications and yield of blood cultures in hospitalized medical patients. J Hosp Med. 2016;11(5):336-340.
11. Matzek LJ, LeMahieu MJ, Kor DJ, et al. A contemporary analysis of phlebotomy and iatrogenic anemia development throughout hospitalization in critically ill adults. Anesth Analg. 2022;135(3):501- 510.
12. Wiener-Well Y, Levin PD, Assous MV, et al. The use of a diversion tube to reduce blood culture contamination: A "real-life" quality improvement intervention study. Am J Infect Control. 2023.
13. Frota OP, Silva RM, Ruiz JS, et al. Impact of sterile gloves on blood-culture contamination rates: A randomized clinical trial. Am J Infect Control. 2022;50(1).
14. Hoque F. Patient Experience as a National Quality Metric. Am J Med Qual. 2025;40(5):246. doi:10.1097/JMQ.0000000000000251
15. Szewczyk T, Hoque F. Improving Patient Experience in Healthcare. J Brown Hosp Med. 2026;5(1):147405. Published 2026 Jan 1. doi:10.56305/001c.147405