Interdisciplinary Bedside Rounds to Advance Interprofessional Communication for Patient-Centered Care
Karen Bri Dale ,Farzana Hoque
1 Saint Louis University School of Medicine, St. Louis, Missouri, USA
2 Associate Professor of Medicine, Saint Louis University School of Medicine, Saint Louis, MO.
Corresponding Authors: Farzana Hoque
Correspondence: MD, MSHA, MRCP, FACP, FRCP, Associate Professor of Medicine, Saint Louis University School of Medicine, 1201 S Grand Blvd, St. Louis, MO 63104Interdisciplinary bedside rounds (IBRs) have emerged as a transformative model for advancing interprofessional communication and delivering patient-centered care — yet their adoption remains inconsistent, and their full potential largely unrealized across inpatient medicine. As healthcare systems face mounting pressure to improve safety, care coordination, and patient experience simultaneously, the structure of daily hospital rounds has never been more consequential. Traditional physician-led rounds, while deeply embedded in clinical culture, carry well-documented limitations — hierarchical communication, restricted patient participation, and fragmented decision-making — that increasingly fall short of modern standards for collaborative, equitable care. This narrative review critically examines five major rounding models — traditional medical rounds, multidisciplinary rounds, IBR, structured interdisciplinary bedside rounds (SIBR), and trio rounds — evaluating each through the lens of interprofessional communication, patient experience, and clinical outcomes. Rather than advocating for a single universal model, this review reveals that optimal rounding is context-dependent, shaped by institutional resources, clinical complexity, and team composition. By synthesizing the current evidence and defining the distinct role of each rounding model, this review offers a practical framework for clinicians and healthcare leaders seeking to elevate interprofessional collaboration — and outlines the research priorities needed to standardize IBR implementation across diverse inpatient settings.
Keyword: Interdisciplinary bedside rounds Patient-centered Care Physician-patient relationships Patient experience Interprofessional Communication Physician Communication
Interdisciplinary Bedside Rounds to Advance Interprofessional Communication for Patient-Centered Care
Karen Bri Dale ,Farzana Hoque
1 Saint Louis University School of Medicine, St. Louis, Missouri, USA
2 Associate Professor of Medicine, Saint Louis University School of Medicine, Saint Louis, MO.
Corresponding Authors: Farzana Hoque
Correspondence: MD, MSHA, MRCP, FACP, FRCP, Associate Professor of Medicine, Saint Louis University School of Medicine, 1201 S Grand Blvd, St. Louis, MO 63104
INTRODUCTION
Interdisciplinary bedside rounding (IBR) is a patientcentered approach that emphasizes real-time interprofessional communication and collaboration. IBR has become an integral component of daily practice for hospitalists across a wide range of healthcare settings — including academic medical centers and community hospitals because it aligns with the core priorities of inpatient care: safety, efficiency, shared decision-making, and patient engagement. Historically, hospital ward rounds were primarily physician-led and often conducted away from the patient, whether at the bedside with limited team participation or in hallways and conference rooms. This traditional model has been criticized for reinforcing hierarchy, restricting input from non-physician team members, and creating an environment that may feel intimidating or disempowering for patients.1 In response to these limitations, five rounding models have emerged in modern hospital medicine: traditional medical rounds, multidisciplinary rounds, interdisciplinary bedside rounds, and trio rounds.
Definitions and Types of Rounds
Traditional medical rounds reflect the conventional physician-led model, typically involving attending physicians, resident physicians, and medical students, with a focus on medical education. Depending on physician preference and clinical context, discussions may occur at the bedside or elsewhere on the unit. In many settings, non-physician team members are not consistently included in the rounding process, which may limit interdisciplinary input into patient care.1
Multidisciplinary rounds (MDR) are structured, scheduled meetings that bring together representatives from multiple healthcare disciplines — including nurses, physical and occupational therapists, dietitians, pharmacists, case managers, and physicians — to review patient status, diagnoses, and treatment plans.2 These rounds typically occur away from the bedside and focus on logistical coordination, including discharge planning, resource allocation, and post-acute care arrangements. This format is particularly valuable in settings where efficient bed management and interdepartmental coordination are priorities.3,4
Interdisciplinary bedside rounding (IBR) is a patientcentered model in which physicians, nurses, pharmacists, case managers, social workers, and trainees conduct rounds together at the bedside (Figure 1).4,5 IBR has demonstrated improvements in care coordination, communication quality, and active patient and family involvement in shared decision-making. This format is frequently used in academic medical centers, where bedside teaching is integrated into interprofessional practice. Bedside presentations are a core feature of IBR and have been associated with improved clinician– patient interactions and higher satisfaction with care.6
Structured Interdisciplinary Bedside Rounds (SIBR) represent a standardized adaptation of IBR developed to improve efficiency and reduce variability in communication.8.9 SIBR employs a predefined sequence of presenters, clearly defined team roles, and structured checklists to support comprehensive and time-effective rounds.8,9 This format ensures participation from all key disciplines while maintaining a predictable and respectful process for patients and families.8
Trio rounds are a hybrid approach to interdisciplinary bedside rounding commonly seen in smaller community settings. The original trio consisted of the physician, bedside nurse, and patient; however, this model has since been expanded to include a case manager or social worker in some healthcare systems.9,10 Although smaller in scope than full interdisciplinary teams, trio rounds can achieve meaningful improvements in patient outcomes, interprofessional communication, and the integration of clinical care, nursing care, and discharge planning.10 This format offers a practical balance between efficiency and collaboration, though it may be best suited to community settings where staffing is limited and the medical education component of interdisciplinary rounding for trainees is less emphasized.
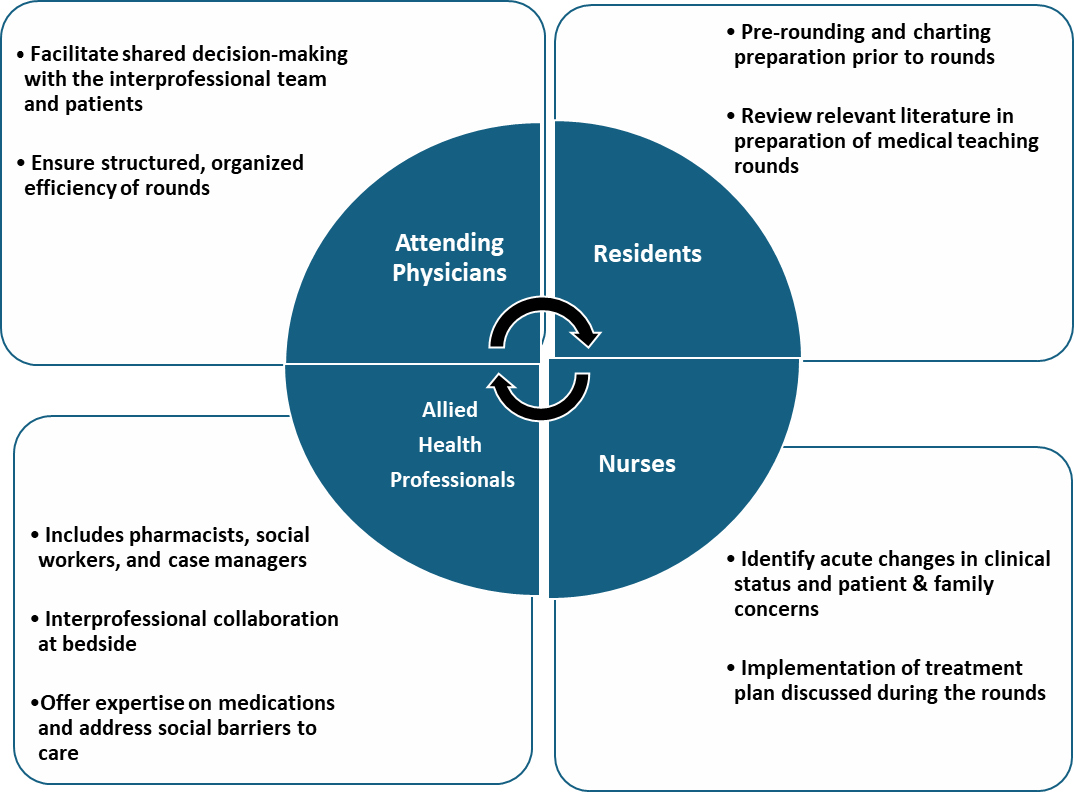
Figure 1: Interdisciplinary bedside rounds workflow and individual responsibilities
Benefits of Each Rounding Model
Traditional medical rounds emphasize medical education and evidence-based clinical discussion.12 Although typically physician-led and conducted away from the bedside, this format can be adapted to include bedside interactions that promote patient-centered communication and rapport. Traditional rounds allow for efficient daily updates to patients and caregivers from a single primary team and remain highly adaptable to the fast-paced workflow of current healthcare landscape.
Multidisciplinary rounds provide a structured environment for interprofessional communication and systematic updates on patient status across healthcare disciplines. The inclusion of both physicians and nurses promotes shared understanding, improves care coordination, and enhances communication quality.13 This model has been associated with reduced length of stay, improved discharge planning, and greater physician engagement and accountability.14
Interdisciplinary bedside rounds emphasize active patient engagement and shared decision-making by bringing key members of the care team — including physicians, nurses, pharmacists, case managers, social workers, and trainees — to the patient's bedside.4,5 In academic centers, this approach also supports real-time medical education. IBR has been shown to strengthen clinician–patient relationships, increase patient and family satisfaction, and improve overall patient safety.5
Trio rounds are well suited to environments with limited staffing resources, offering an adaptable model of bedside rounding with active inclusion of patient, primary nurse and physician. Although the available literature is limited as it a relative new concept, trio rounds may achieve improvements in patient experience and outcomes comparable to IBR, including gains in patient safety, length of stay, interprofessional communication, and satisfaction with care.10 This model can enhance care coordination without the logistical demands of full interdisciplinary rounding.
Challenges of Each Rounding Model
The hierarchical structure of traditional rounds may limit participation from allied health professional team members and discourage patients from speaking up.15 Rounding duration can vary widely due to interruptions, physical distance between patient rooms, competing educational demands, and individual attending practice styles.16 These variations can create communication gaps and disrupt continuity of care, particularly when key clinical disciplines are not consistently represented.15 Traditional rounds may be most appropriate in academic medical centers where physician-led teaching is prioritized and scheduling flexibility for trainees is required.
Because multidisciplinary rounds traditionally occur away from the bedside, they often exclude patients and families from care discussions, limiting transparency and shared decision-making. This separation can generate misunderstandings about treatment goals, discharge planning, or medication changes — especially for patients with complex medical or social needs. Multidisciplinary rounds may also reinforce hierarchical communication patterns, with physicians leading the dialogue while other team members contribute to discipline-specific rather than integrated ways, reducing collaborative problem-solving. Furthermore, the absence of real-time patient involvement may delay recognition of health literacy barriers, cultural preferences, or resource limitations, contributing to preventable delays, readmissions, or lower satisfaction with care. Multidisciplinary rounds are particularly useful in highvolume inpatient units where centralized care planning, discharge coordination, and resource allocation are operational priorities.
Substantial variation in IBR team composition creates barriers to consistent implementation and outcome evaluation across institutions.14 A frequent critique is that bedside rounds increase rounding time, particularly when roles are unclear or discussions become unfocused.16 Inefficiencies may arise from unclear expectations, conversational drift, or interruptions from clinical workflow demands. Structured formats such as SIBR attempt to address these challenges through predefined checklists, sequenced presentation formats, and standardized communication expectations to improve efficiency and ensure participation from all team members.17,18,19 Interdisciplinary bedside rounds are well suited to patient-centered environments with high clinical complexity — such as intensive care units or specialty services — where real-time collaboration and shared decision-making are essential to safe care.
Trio rounds, while adaptable to smaller hospital settings, may lack input from pharmacists, therapists, or dietitians, limiting the depth of interdisciplinary insight in complex cases. Coordinating nurse and physician schedules for daily rounds presents an additional implementation barrier.9, 10 As most of these rounds happen in the morning, where are nurses are responsible to take hands-off and passing meds to patients, thoughtful communication between physicians and nurses are critical for trio rounds consistency. Trio rounds may be most effective in community-based hospitals where full interdisciplinary participation is not feasible but structured communication among core clinicians and the patient remains essential.
Impact of Interdisciplinary Bedside Rounds on Patient Experience
Strengthening Physician–Patient Relationships
Interdisciplinary bedside rounds serve as a critical foundation for strengthening clinician–patient relationships when structured around patient-centered care. Wang et al., in a multidisciplinary retrospective study, found that interdisciplinary bedside rounding enhanced physician–patient relationships by improving nurse–physician communication and integrating shared discussion at the bedside.19 Patient experience is shaped by the interplay between the healthcare system, the quality of communication among team members and patients, and the overall treatment plan. Improved patient experience has downstream effects on financial performance, medication adherence, patient safety, and clinical outcomes.19,20,21 Clear role expectations for each team member are essential to optimizing patient experience and interprofessional collaboration. Although these expectations vary by institution and study, common elements include pre-rounding by resident and student physicians, timely nurse notification of clinical changes, minimization of medical jargon during patient discussions, and designated time for input from pharmacists, case managers, and other team members.22,23 Studying the impact of interdisciplinary rounds on physician–patient relationships is challenging given variability in team composition; many studies examine interprofessional collaboration without defining the components required for maximal benefit. Vundi et al. demonstrated that teams including physicians, nurses, pharmacists, and case managers or social workers were more likely to incorporate patient-centered considerations — such as financial constraints, medication access, and discharge readiness — into clinical decision-making.22 Across the literature, active patient participation consistently emerges as the primary driver of strong clinician–patient relationships. Among communication elements, patient-centered language and reduced medical jargon exert the strongest influence on clinician–patient rapport. When demographic factors such as age, gender, and race are controlled, the most significant predictor of relationship strength is the physician's ability to align communication with the patient's health literacy level. 23 Mastalerz et al. identified four essential communication components to support engagement during bedside rounds: patient-centered language, clearly defined team roles, standardized presentation of information for both patients and clinicians, and real-time feedback with patients and families.24
Interdisciplinary bedside rounds promote empathy by helping the team understand the patient's lived experience, values, and barriers in real time — reducing assumptions and guiding a care plan that is compassionate, culturally informed, and truly patientcentered.25 Structured interdisciplinary bedside rounds help to reduce variability in rounding time per patient, promoting efficiency without compromising interaction quality. Many IBR implementation studies utilized rounding checklists to ensure communication consistency, enabling teams to maintain efficiency while improving quality.21 The literature broadly supports that when interdisciplinary bedside rounding includes clear role expectations and the appropriate care team members, it reduces rounding interruptions and total rounding time.17,18,19 Interdisciplinary bedside rounding can therefore strengthen clinician–patient relationships and improve patient-centered outcomes without sacrificing efficiency, provided it is executed in a structured, intentional format.
Patient Satisfaction and Perception of Care
Interdisciplinary bedside rounds have been shown to improve patient and family satisfaction as reflected in self-reported experience scores. Patient satisfaction increasingly functions as a proxy outcome for patientcentered care, with healthcare systems using these measures to evaluate communication quality, shared decision-making, and trust. Even in high-acuity settings such as intensive care units, structured interdisciplinary bedside rounds have been associated with enhanced team communication, increased educational opportunities for trainees, and improved patient perceptions of care.26 When clinicians sat at the patient's bedside during discussion, patients perceived the team as spending more time with them, resulting in higher satisfaction scores.25 The presence of family members during rounds has been associated with increased reported satisfaction with care.27,28 Interdisciplinary bedside rounds also enable physicians to tailor care based on social determinants of health.29 For example, when a social worker identifies financial constraints, the physician can prescribe more affordable medications or adjust the regimen accordingly. If food insecurity or limited home support is identified, the team can connect the patient to resources such as Meals on Wheels and arrange home health services to support a safe and realistic discharge plan.29 A study showed that patient and caregiver awareness of multidisciplinary rounding (MDR) times—and subsequent participation in MDR— is associated with fewer adverse events, shorter average length of stay, and higher satisfaction.30 By creating a structured space for discussion and shared decisionmaking, interdisciplinary bedside rounds can reduce uncertainty, improve emotional support, and ease the burden on family members acting as surrogate decision-makers.31 Cypress et al. conducted a qualitative exploratory study identifying barriers that limit active patient and family participation during bedside rounds.32 At the individual level, patients and families reported gaps between the medical information provided and their own health literacy. At the interpersonal level, they described unclear leadership and inconsistent support among team members. At the organizational level, the absence of formal policies supporting family engagement restricted participation.32 Addressing these barriers is essential to maximizing the impact of interdisciplinary bedside rounds on patient satisfaction and patientcentered care
Enhancing Team-based Communication and Patient Safety
Structured interdisciplinary bedside rounds (SIBR) were associated with significantly higher staff-reported scores for teamwork, communication, understanding of the day’s plan, safety, efficiency, and job satisfaction compared with traditional physician-centric rounds.33 These gains suggest improved communication-related markers of quality and safety alongside improved nursing satisfaction.33 However, the current literature is limited by variations in study design, team composition, and institutional context — such as academic versus community hospital settings — which restrict generalizability. Sunkara et al. found that interdisciplinary bedside rounds in large academic hospitals did not significantly affect hospital length of stay or 30-day readmission rates, but did significantly reduce 7-day readmissions.34 Structured interdisciplinary bedside rounds were also associated with improved clinician-reported outcomes, with participating physicians, nurses, pharmacists, and case managers describing higher satisfaction and better educational and professional experience, including perceived gains in clinical skills and team-based practice.35,36 Clay-Williams et al. further demonstrated a reduction in overall cost of stay associated with interdisciplinary bedside rounds in a large tertiary hospital, indicating both clinical and financial benefit.37 Basic et al. reported an association between twice-weekly structured interdisciplinary bedside rounds and a reduction in inpatient falls among older adults, though causality was not fully established.38 Radhakrishnan et al. demonstrated that incorporating structured checklists into interdisciplinary bedside rounds significantly reduced central-line-associated bloodstream infections (CLABSIs), catheter-associated urinary tract infections, and length of stay.39 Linam et al. examined interdisciplinary bedside rounds in neonatal and pediatric intensive care units and found that when infection prevention was emphasized during rounds, the incidence of CLABSIs decreased.40 These findings highlight the potential of interdisciplinary rounds to improve outcomes when intentionally designed to target specific safety priorities. Future research with larger sample sizes and clearly defined primary outcomes is needed to better establish the causal effects of IBR on preventable harm.
Conclusion
Interdisciplinary bedside rounds (IBRs) are pivotal for cohesive interprofessional communication, strengthening clinician–patient relationships, and promoting care coordination. When physicians, nurses, pharmacists, social workers, and case managers converge at the bedside with clearly defined roles and a structured communication framework, IBR consistently delivers higher patient and family satisfaction, measurable improvements in patient safety, and meaningful reductions in preventable adverse events — including CLABSIs, inpatient falls, and early readmissions. Central to IBR's impact is the patient experience. Active engagement in shared decisionmaking fosters greater trust, improved understanding of treatment goals, and a stronger sense of being heard — driving better medication adherence, safer care transitions, and fewer readmissions. IBR further creates an irreplaceable opportunity to address social determinants of health in real time, ensuring every care plan is clinically sound, equitable, and practically achievable. When implemented within a structured framework such as SIBR, these rounds enhance efficiency, reduce communication variability, and improve satisfaction across all disciplines involved in care. To advance the field, future research should prioritize the development and validation of standardized IBR implementation frameworks adaptable across diverse inpatient settings. Prospective, multicenter studies with clearly defined outcomes — including patient safety endpoints, workflow efficiency, health equity metrics, and patient experience — are needed to establish the causal benefits of IBR and guide evidence-based adoption. As healthcare systems continue to emphasize value-based, patient-centered care, interdisciplinary bedside rounds offer a scalable and impactful model for transforming how teams communicate, collaborate, and deliver care at the bedside.
1. Walton V, Hogden A, et al. Clinicians’ perceptions of rounding processes and effectiveness of clinical communication. J Eval Clin Pract. 2020;26(3):801- 811. doi:10.1111/jep.13248
2. Srinivas V, Choubey U, Motwani J, et al. Synergistic strategies: optimizing outcomes through a multidisciplinary approach to clinical rounds. Proc (Bayl Univ Med Cent). 2024;37(1):144-150. doi:10.1080/08998280.2023.2274230
3. Valente R, Santori G, Stanton L, Abraham A, Thaha MA. Introducing a structured daily multidisciplinary board round to safely enhance surgical ward patient flow in the bed shortage era: a quality improvement research report. BMJ Open Qual. 2023;12(1): e001669. doi:10.1136/bmjoq-2021-001669
4. Hoque F. Benefits & framework of interprofessional collaboration in clinical practice. JBMANA. 2023 ;2(1):1-8.
5. Heip T, Van Hecke A, Malfait S, Van Biesen W, Eeckloo K. The effects of interdisciplinary bedside rounds on patient centeredness, quality of care, and team collaboration: a systematic review. J Patient Saf. 2022;18(1):e40-e44. doi:10.1097/PTS.00000000000 00695
6. UNC School of Medicine. Implementing patientcentered multidisciplinary bedside rounds. Published 2019. Accessed July 31, 2025.
7. Schwartz JI, Gonzalez-Colaso R, Gan G, et al. Structured interdisciplinary bedside rounds improve interprofessional communication and workplace efficiency among residents and nurses on an inpatient internal medicine unit. J Interprof Care. 2024;38 (3):427-434. doi:10.1080/13561820.2020.1863932
8. Aldamouk A. The impact of patient-centered, structured interdisciplinary bedside rounds on medical staff satisfaction, education, and experience. Cureus. 2024;16(12):e76412. doi:10.7759/cureus. 76412
9. Epling B, Askelrod H. Utility of trio rounds and barriers to their implementation. Poster. George Washington University, School of Medicine and Health Sciences Poster Presentations. Published May 1, 2019. Accessed July 31, 2025.
10. Association of Rehabilitation Nurses. Trio-rounding: perception of benefits and challenges by rehabilitation nurses and physicians. Newswise. Published September 10, 2020. Accessed July 31, 2025.
11. Noorani M. The ward round: friend or foe in postgraduate training? A grounded theory study of residents’ perspectives. Med Educ Online. 2022;27(1):2101180. doi:10.1080/10872981.2022. 2101180
12. Babael A. Bridging the gap: how multidisciplinary rounds boost communication between nurses and physicians in the intensive care unit. J Nurs Rep Clin Pract. 2024;2(3). doi:10.32598/JNRCP.2402.1018
13. Nimmagadda K, Pancrazi S, Martino A, et al. Virtual multidisciplinary rounds to reduce length of stay, decrease variation, and promote accountability. Jt Comm J Qual Patient Saf. 2023;49(9):450-457. doi:10.1016/j.jcjq.2023.04.006
14. O’Hare JA. Anatomy of the ward round. Eur J Intern Med. 2008;19(5):309-313. doi:10.1016/j.ejim.2007. 09.016
15. Al Halabi A, Habas ESr, Farfar KL, et al. Time spent on medical round activities, distance walked, and time-motion in the general medicine department at Hamad General Hospital in Qatar. Cureus. 2023;15(4):e37935. doi:10.7759/cureus.37935
16. Huang KTL, et al. All together now: impact of a regionalization and bedside rounding initiative on the efficiency and inclusiveness of clinical rounds. J Hosp Med. 2017;12(3):150-156. doi:10.12788/jhm. 2696
17. Lopez M, et al. Impacting satisfaction, learning, and efficiency through structured interdisciplinary rounding in a pediatric intensive care unit: a quality improvement project. Pediatr Qual Saf. 2019;4(3):e176. doi:10.1097/pq9.0000000000000176
18. Making patients part of the team helps hospital cut LOS, boost HCAHPS scores. Hosp Case Manag. 2017;25(3):34,39
19. Wang J, et al. Improving nurse-physician bedside communication using a patient experience quality improvement pilot project at an academic medical center. Cureus. 2024;16(3):e55976. doi:10.7759/ cureus.55976
20. Hoque F. Patient Experience as a National Quality Metric. Am J Med Qual. 2025;40(5):246. doi:10.1097/ JMQ.0000000000000251
21. Szewczyk T, Hoque F. Improving Patient Experience in Healthcare. J Brown Hosp Med. 2026;5(1):147405. Published 2026 Jan 1. doi:10.56305/001c.147405
22. Vundi N, et al. Implementation and function of interdisciplinary rounds: an observational multisite hospital study from project ACHIEVE. J Hosp Med. 2023;18(3):224-233. doi:10.1002/jhm.13062
23. Lehmann LS, et al. The effect of bedside case presentations on patients’ perceptions of their medical care. N Engl J Med. 1997;336(16):1150-1155. doi: 10.1056/NEJM199704173361606
24. Mastalerz KA, et al. A qualitative study of patient and interprofessional healthcare team member experiences of bedside interdisciplinary rounds at a VA: language, teamwork, and trust. J Gen Intern Med. 2025 ;40(3):538-546. doi:10.1007/s11606-024- 09124-8
25. Hoque F. Empathy in healthcare: Harmonizing curing and caring in healthcare. J Hosp Med. 2025; 20: 517- 520. doi:10.1002/jhm.13540
26. Cao V, et al. Patient-centered structured interdisciplinary bedside rounds in the medical ICU. Crit Care Med. 2018;46(1):85-92. doi:10.1097/CCM .0000000000002807
27. Sisterhen LL, et al. Defining family-centered rounds. Teach Learn Med. 2007;19(3):319-322. doi:10.1080/ 10401330701366812
28. Kuo DZ, et al. Family experiences and pediatric health services use associated with family-centered rounds. Pediatrics. 2012;130(2):299-305. doi:10.1542/peds .2011-2623
29. Vrtikapa K, Hoque Urmy F, Hoque F. Social Determinants of Health: The Impact of This Overlooked Vital Sign. J Brown Hosp Med. 2025;4(3):138072. Published 2025 Jul 1. doi:10.56305/001c.138072
30. Qureshi A, et al. When is my care team rounding? A simple signage intervention to increase awareness of rounding times. J Patient Exp. 2021;8:23743 735211007358. doi:10.1177/23743735211007358
31. Hoque F. Shared decision making: a win-win situation for both patients and physicians. American Journal of Hospital Medicine. 2023;7(2).
32. Cypress B, et al. Healthcare professionals’ perspective of the facilitators and barriers to family engagement during patient-and-family-centered-care interdisci-plinary rounds in intensive care unit: a qualitative exploratory study. Intensive Crit Care Nurs. 2024;82:103636. doi:10.1016/j.iccn.2024.103 636
33. Gausvik C, et al. Structured nursing communication on interdisciplinary acute care teams improves perceptions of safety, efficiency, understanding of care plan and teamwork as well as job satisfaction. J Multidiscip Healthc. 2015;8:33-37. doi:10.2147/ JMDH.S72623
34. Sunkara PR, et al. Impact of structured interdisciplinary bedside rounding on patient outcomes at a large academic health centre. BMJ Qual Saf. 2020;29(7):569-575. doi:10.1136/bmjqs2019-009936
35. Aldamouk A. The Impact of Patient-Centered, Structured Interdisciplinary Bedside Rounds on Medical Staff Satisfaction, Education, and Experience. Cureus. 2024;16(12):e76412. Published 2024 Dec 26. doi:10.7759/cureus.76412
36. Wickersham A, et al. Making room at the bedside: improving communication alongside medical education through interdisciplinary rounds. Am J Med Qual. 2021;36(1):42-48. doi:10.1177/10628606 20908058
37. Clay-Williams R, et al. Improving teamwork and patient outcomes with daily structured interdisciplinary bedside rounds: a multimethod evaluation. J Hosp Med. 2018;13(5):311-317. doi:10.12788/jhm.2850
38. Basic D, Huynh ET, Gonzales R, Shanley CG. TwiceWeekly Structured Interdisciplinary Bedside Rounds and Falls among Older Adult Inpatients. J Am Geriatr Soc. 2021;69(3):779-784. doi:10.1111/jgs.17007
39. Radhakrishnan NS, et al. Prospective application of the interdisciplinary bedside rounding checklist “TEMP” is associated with reduced infections and length of hospital stay. BMJ Open Qual. 2022 ;11(4):e002045. doi:10.1136/bmjoq-2022-002045
40. Linam M, et al. Initiation of interdisciplinary prevention rounds: decreasing CLABSIs in critically ill children. Antimicrob Steward Healthc Epidemiol. 2024;4(1):e80. doi:10.1017/ash.2024.55